

Bilirubin gates the TRPM2 channel as a direct agonist to exacerbate ischemic brain damage
- PMID: 36921602
- PMCID: PMC10191619
- DOI: 10.1016/j.neuron.2023.02.022
Bilirubin gates the TRPM2 channel as a direct agonist to exacerbate ischemic brain damage
Abstract
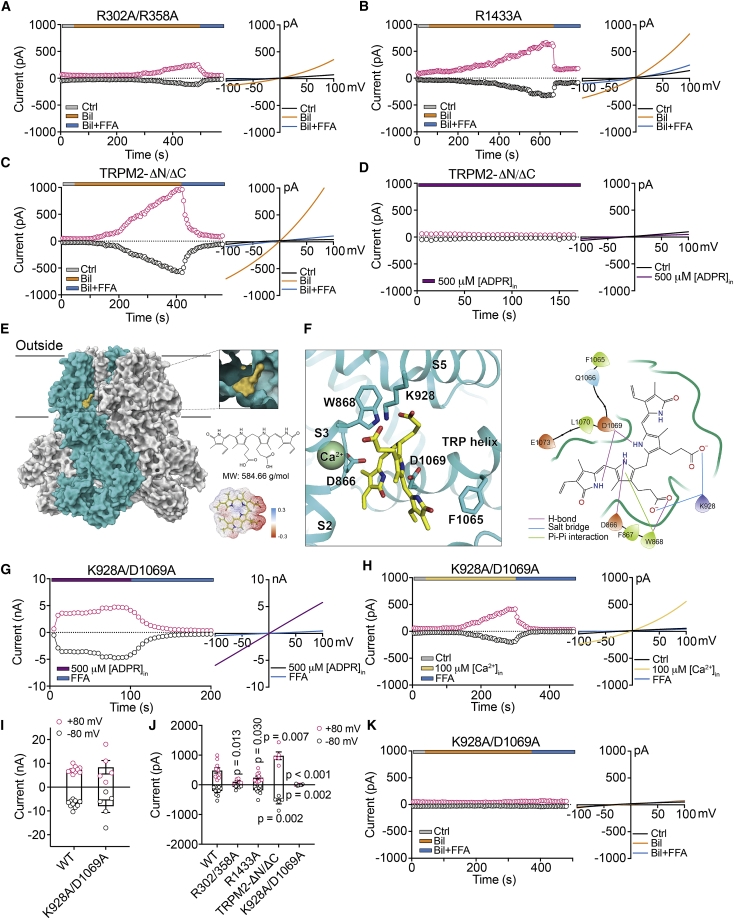
Stroke prognosis is negatively associated with an elevation of serum bilirubin, but how bilirubin worsens outcomes remains mysterious. We report that post-, but not pre-, stroke bilirubin levels among inpatients scale with infarct volume. In mouse models, bilirubin increases neuronal excitability and ischemic infarct, whereas ischemic insults induce the release of endogenous bilirubin, all of which are attenuated by knockout of the TRPM2 channel or its antagonist A23. Independent of canonical TRPM2 intracellular agonists, bilirubin and its metabolic derivatives gate the channel opening, whereas A23 antagonizes it by binding to the same cavity. Knocking in a loss of binding point mutation for bilirubin, TRPM2-D1066A, effectively antagonizes ischemic neurotoxicity in mice. These findings suggest a vicious cycle of stroke injury in which initial ischemic insults trigger the release of endogenous bilirubin from injured cells, which potentially acts as a volume neurotransmitter to activate TRPM2 channels, aggravating Ca2+-dependent brain injury.
Keywords: TRPM2; agonist; hyperbilirubinemia; stroke; volume neurotransmitter.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests We have filed a patent application for the bilirubin-binding cavity on the TRPM2 channel for developing therapeutics to treat brain injury in stroke and jaundice.
Figures








References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
