

Frailty in Patients with Chronic Graft-versus-Host Disease
- PMID: 36921916
- PMCID: PMC10239364
- DOI: 10.1016/j.jtct.2023.03.010
Frailty in Patients with Chronic Graft-versus-Host Disease
Abstract
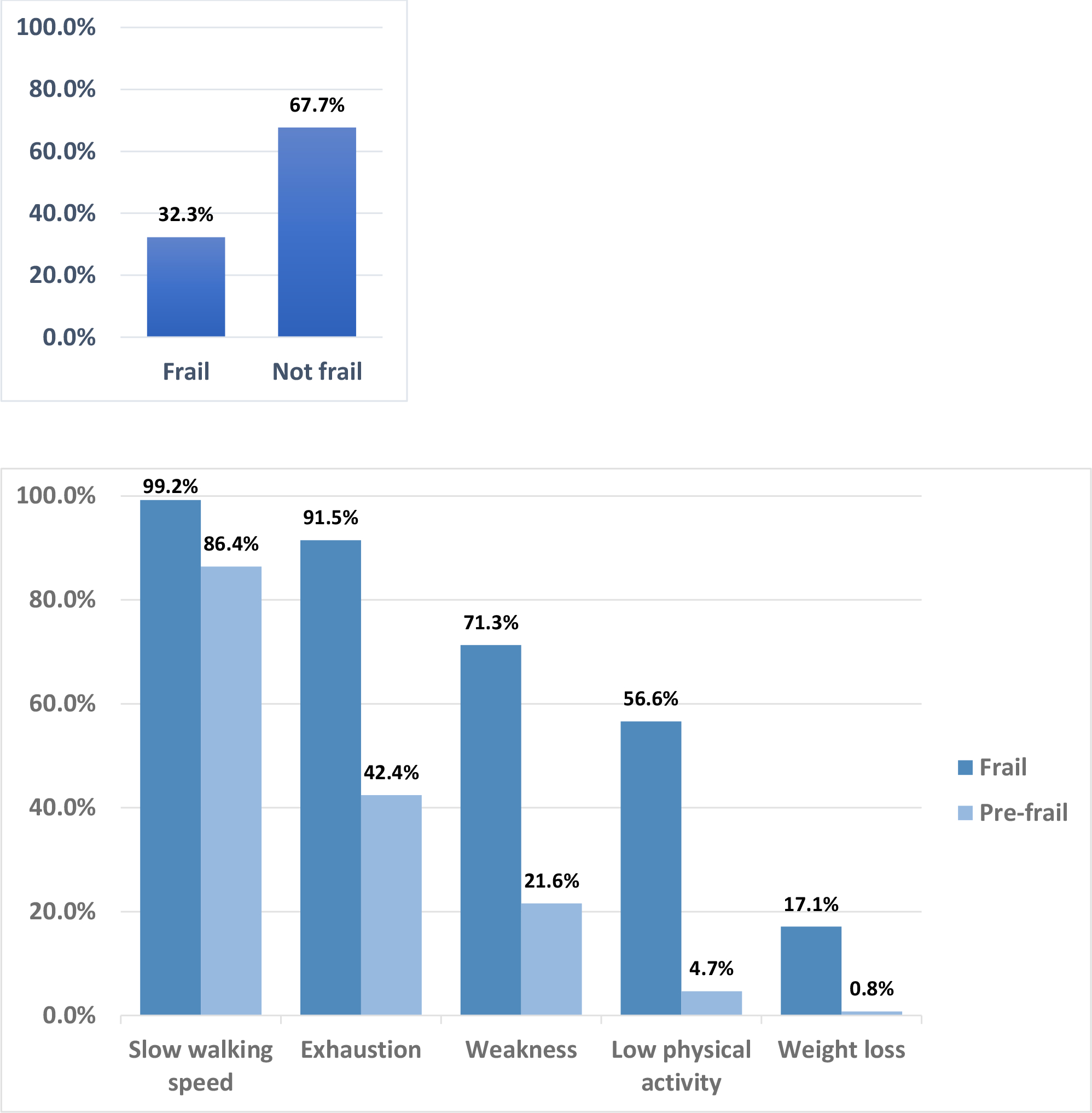
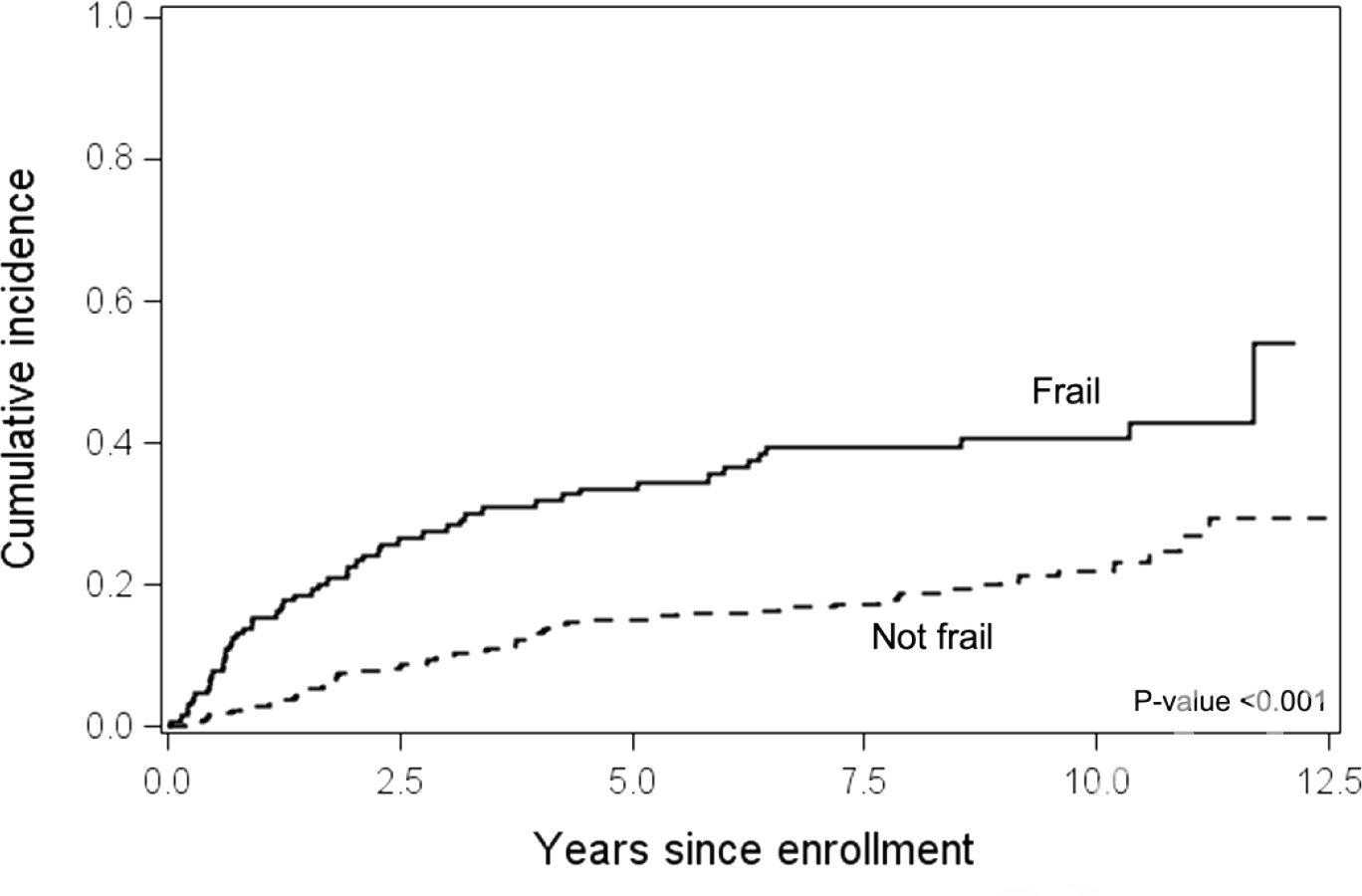
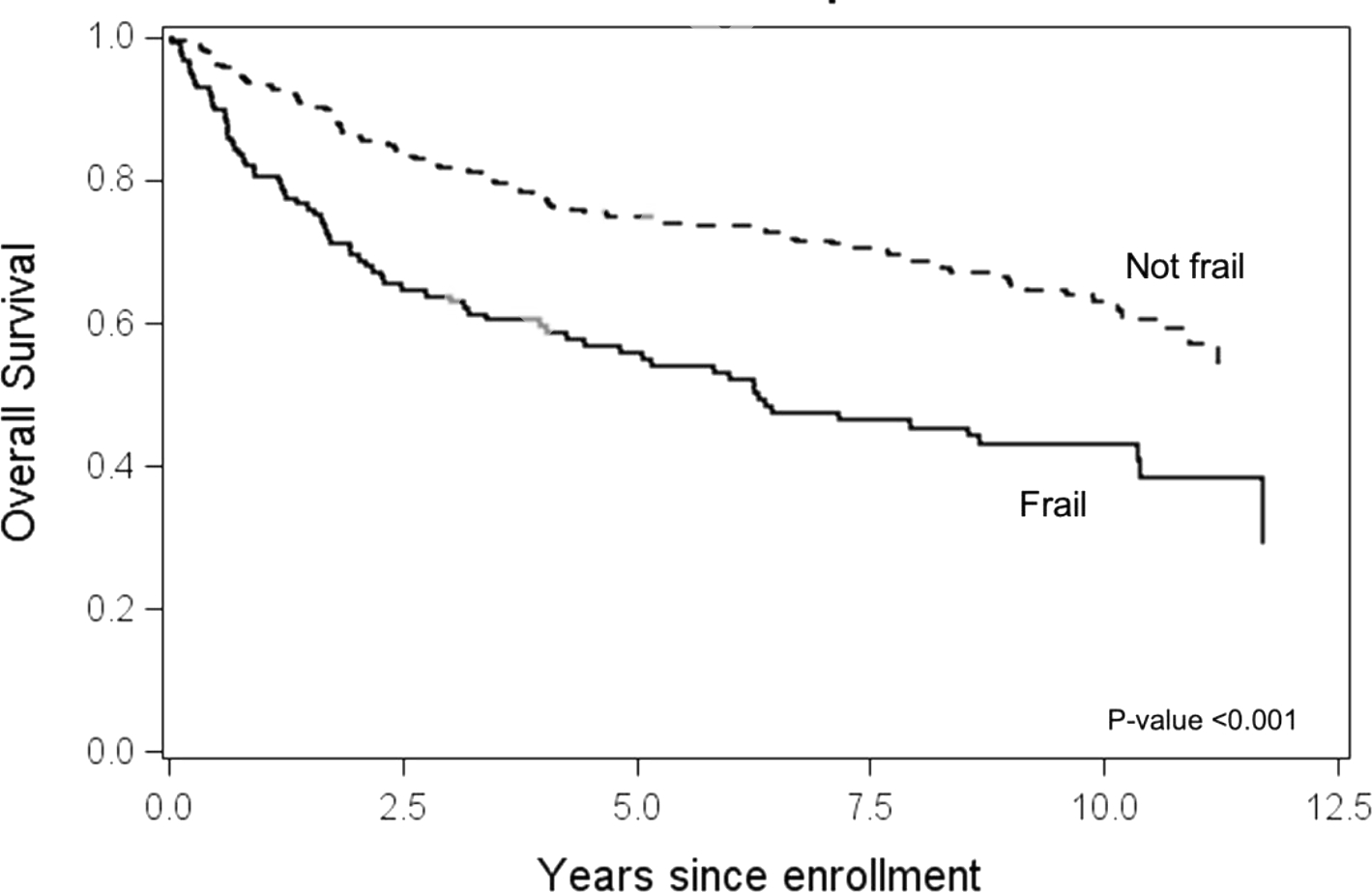
Frailty is an increasingly recognized clinical diagnosis associated with high risk of disability and mortality. Frailty in patients after hematopoietic cell transplantation (HCT) is associated with increased nonrelapse mortality (NRM) and decreased overall survival (OS). Frailty has not been studied extensively in patients with chronic graft-versus-host disease (cGVHD). The objectives of the present study were to assess the prevalence and clinical correlates of frailty and the association of frailty with NRM and OS in patients enrolled in the Chronic GVHD Consortium. Patients were characterized as frail if they met the Fried definition of ≥3 of the following criteria at enrollment: unintentional weight loss, exhaustion, slow walking speed, low physical activity, and weakness. Frailty was assessed retrospectively using surrogate measures for the 5 domains of frailty. Frailty, cGVHD organ scores, and patient-reported outcomes were measured at the time of enrollment. The study included 399 patients from 9 centers in the United States, with 32% characterized as frail and 68% as not frail. The median duration of follow-up from enrollment was 9 years (interquartile range, 7 to 11 years). Frail patients were more likely to be older (P = .004), to have a lower Karnofsky Performance Status (P < .001), to have severe cGVHD (P < .001), and to have gastrointestinal (P < .001), liver (P = .04), or lung cGVHD (P = .002). In a multivariable analysis, older age, increased cGVHD global severity, and thrombocytopenia were statistically significantly associated with frailty when cGVHD organ involvement was excluded. A separate analysis excluding cGVHD severity and including organ involvement showed that lung and liver cGVHD and older age were associated with frailty. Neither corticosteroid use at the time of enrollment nor the maximum recorded dose of corticosteroids before enrollment was associated with frailty. Frail patients had higher NRM than nonfrail patients (P < .001), with a 10-year cumulative incidence of 41% (95% confidence interval [CI], 32% to 49%) versus 22% (95% CI, 17% to 28%). Reciprocally, frailty also was associated with a significantly lower OS (P < .001), with a 10-year OS of 43% (95% CI, 35% to 53%) in frail patients versus 63% (95% CI, 57% to 69%) in nonfrail patients. In multivariable analysis that included the individual domains of frailty, weakness, low physical activity, and slow walking speed were associated with survival. Frail patients also had worse scores on various measures of patient-reported outcomes, including the Short Form (SF)-36, the Lee Symptom Scale, and the trial outcome of the Functional Assessment of Cancer Therapy-Bone Marrow Transplantation (FACT-BMT) index score. Frail patients with cGVHD have significantly worse outcomes than nonfrail patients. Such clinical features as older age and lung and liver cGVHD are associated with frailty. Earlier clinical recognition of frailty in patients with cGVHD may prompt interventions to counteract frailty that could be beneficial for this population.
Keywords: Chronic GVHD; Frailty; Hematopoietic cell transplantation; Patient-reported outcomes.
Copyright © 2023 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors do not have any conflicts of interest
Figures
References
-
- Collard RM, et al., Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc, 2012. 60(8): p. 1487–92. - PubMed
-
- Abel GA and Klepin HD, Frailty and the management of hematologic malignancies. Blood, 2018. 131(5): p. 515–524. - PubMed
-
- Buckstein R, et al., Patient-related factors independently impact overall survival in patients with myelodysplastic syndromes: an MDS-CAN prospective study. Br J Haematol, 2016. 174(1): p. 88–101. - PubMed
-
- Fried LP, et al., Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci, 2001. 56(3): p. M146–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
