

Overview of Ultrasound in Dentistry for Advancing Research Methodology and Patient Care Quality with Emphasis on Periodontal/Peri-implant Applications
- PMID: 36922293
- PMCID: PMC10517409
- DOI: 10.1016/j.zemedi.2023.01.005
Overview of Ultrasound in Dentistry for Advancing Research Methodology and Patient Care Quality with Emphasis on Periodontal/Peri-implant Applications
Abstract
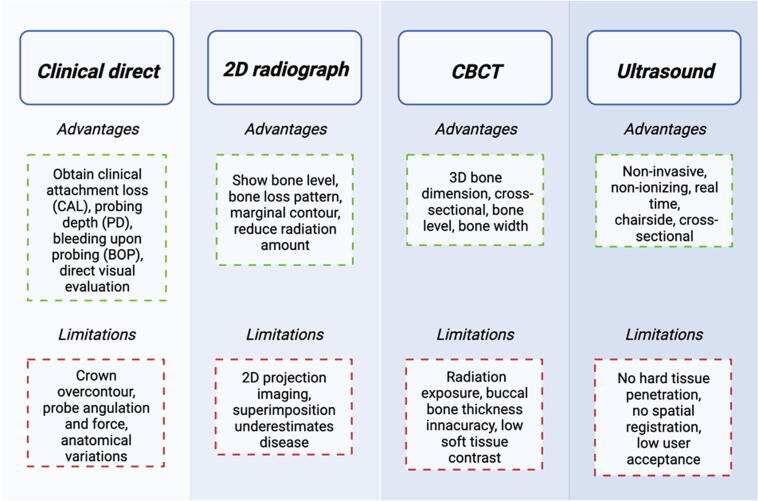
Background: Ultrasound is a non-invasive, cross-sectional imaging technique emerging in dentistry. It is an adjunct tool for diagnosing pathologies in the oral cavity that overcomes some limitations of current methodologies, including direct clinical examination, 2D radiographs, and cone beam computerized tomography. Increasing demand for soft tissue imaging has led to continuous improvements on transducer miniaturization and spatial resolution. The aims of this study are (1) to create a comprehensive overview of the current literature of ultrasonic imaging relating to dentistry, and (2) to provide a view onto investigations with immediate, intermediate, and long-term impact in periodontology and implantology.
Methods: A rapid literature review was performed using two broad searches conducted in the PubMed database, yielding 576 and 757 citations, respectively. A rating was established within a citation software (EndNote) using a 5-star classification. The broad search with 757 citations allowed for high sensitivity whereas the subsequent rating added specificity.
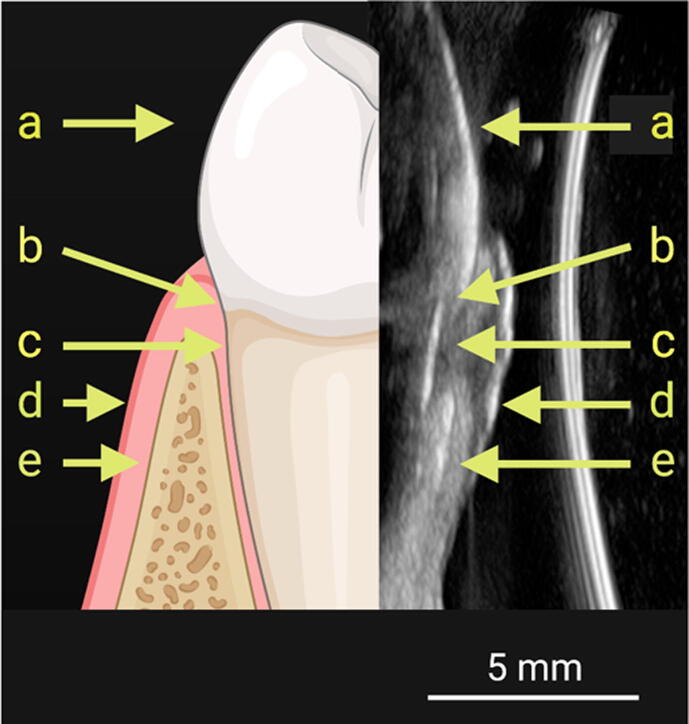
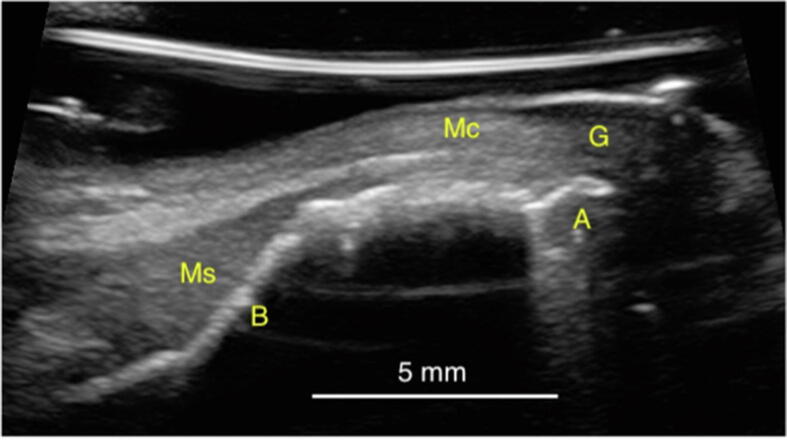
Results: A critical review of the clinical applications of ultrasound in dentistry was provided with a focus on applications in periodontology and implantology. The role of ultrasound as a developing dental diagnostic tool was reviewed. Specific uses such as soft and hard tissue imaging, longitudinal monitoring, as well as anatomic and physiological evaluation were discussed.
Conclusions: Future efforts should be directed towards the transition of ultrasonography from a research tool to a clinical tool. Moreover, a dedicated effort is needed to introduce ultrasonic imaging to dental education and the dental community to ultimately improve the quality of patient care.
Keywords: Dental; Diagnosis; Imaging; Implant; Periodontal; Ultrasound.
Copyright © 2023 The Author(s). Published by Elsevier GmbH.. All rights reserved.
Figures













References
-
- Vanderstuyft T., Tarce M., Sanaan B., Jacobs R., de Faria Vasconcelos K., Quirynen M. Inaccuracy of buccal bone thickness estimation on cone-beam CT due to implant blooming: An ex-vivo study. J Clin Periodontol. 2019;46(11):1134–1143. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
