

Clinical outcome and biomarker assessments of a multi-centre phase II trial assessing niraparib with or without dostarlimab in recurrent endometrial carcinoma
- PMID: 36922497
- PMCID: PMC10017680
- DOI: 10.1038/s41467-023-37084-w
Clinical outcome and biomarker assessments of a multi-centre phase II trial assessing niraparib with or without dostarlimab in recurrent endometrial carcinoma
Abstract
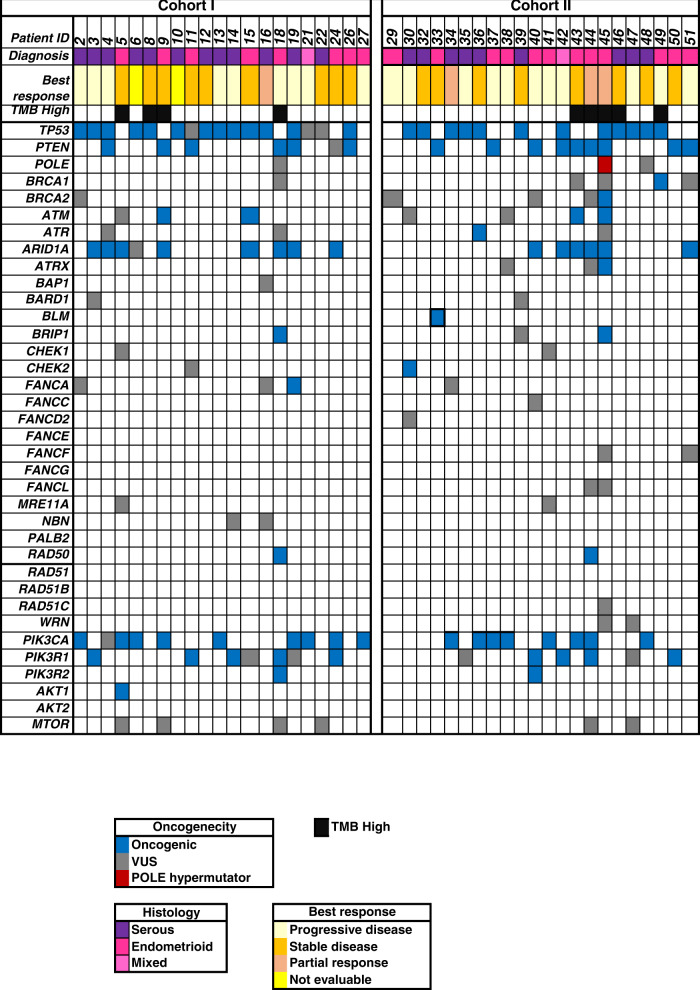
This multi-centre, non-randomized, open-label, phase II trial (NCT03016338), assessed niraparib monotherapy (cohort 1, C1), or niraparib and dostarlimab (cohort 2, C2) in patients with recurrent serous or endometrioid endometrial carcinoma. The primary endpoint was clinical benefit rate (CBR), with ≥5/22 overall considered of interest. Secondary outcomes were safety, objective response rate (ORR), duration of response, progression free survival and overall survival. Translational research was an exploratory outcome. Potential biomarkers were evaluated in archival tissue by immunohistochemistry and next generation sequencing panel. In C1, 25 patients were enrolled, and CBR was 20% (95% CI: 9-39) with median clinical benefit duration of 5.3 months. The ORR was 4% (95% CI: 0-20). In C2, 22 patients were enrolled, and the CBR was 31.8% (95% CI: 16-53) with median clinical benefit duration of 6.8 months. The ORR was 14% (95% CI: 3-35). No new safety signals were detected. No significant association was detected between clinical benefit and IHC markers (PTEN, p53, MMR, PD-L1), or molecular profiling (PTEN, TP53, homologous recombination repair genes). In conclusion, niraparib monotherapy did not meet the efficacy threshold. Niraparib in combination with dostarlimab showed modest activity.
© 2023. The Author(s).
Conflict of interest statement
A.M. received honoraria from AstraZeneca, Clovis, GSK and PharmaMar. N.C.D. declared honoraria from AstraZeneca and Merck. W.J. received honoraria from AstraZeneca and GSK. S.W. declared honoraria from GSK, Merck, AstraZeneca. H.M. is on the advisory board for AstraZeneca, Merck, Essai and GSK. J.L.E. reported speaker fees and advisory board participation for AstraZeneca, GSK and Merck. L.G. declared consulting advisory board fees from AstraZeneca, Alkermes, Merck, Eisai, Eisai-Merck, GSK. She also declared institutional grants from Astra Zeneca, Pfizer, Merck Sharp & Dohme, Kayopharm, Alkermes, ImmunoGen Inc, Roche, Mersana, Esperas, Novocure GmbH, Oncoquest Pharmaceuticals, K-Group Beta Inc. V.B. received honoraria from AstraZeneca and had an uncompensated advisory role in AstraZeneca and GSK. T.S. received honoraria from GSK, AstraZeneca, and Merck. AMO declared uncompensated consulting or advisory role in AstraZeneca and GSK. He has uncompensated relationships with AstraZeneca and Clovis and research funding from AstraZeneca, GSK and Clovis. S.L. declared consulting fees from AstraZeneca, GSK, Merck, Eisai, Novocure, Novartis, Shattuck laboratories. Stephanie Lheureux is principal investigator or co-investigator of different clinical trials with agents from AstraZeneca, Merck, Roche, GSK, Regeneron, Repare Therapeutics, Clovis. The remaining authors declare no other competing interests.
Figures



References
-
- Oaknin A, et al. Clinical activity and safety of the anti-programmed death 1 monoclonal antibody dostarlimab for patients with recurrent or advanced mismatch repair-deficient endometrial cancer: a nonrandomized phase 1 clinical trial. JAMA Oncol. 2020;6:1–7. doi: 10.1001/jamaoncol.2020.4515. - DOI - PMC - PubMed
-
- Oaknin A, et al. LBA36 safety and antitumor activity of dostarlimab in patients (pts) with advanced or recurrent DNA mismatch repair deficient (dMMR) or proficient (MMRp) endometrial cancer (EC): results from GARNET. Ann. Oncol. 2020;31:S1166. doi: 10.1016/j.annonc.2020.08.2266. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
