

Evaluation and deployment of isotype-specific salivary antibody assays for detecting previous SARS-CoV-2 infection in children and adults
- PMID: 36922542
- PMCID: PMC10016188
- DOI: 10.1038/s43856-023-00264-2
Evaluation and deployment of isotype-specific salivary antibody assays for detecting previous SARS-CoV-2 infection in children and adults
Abstract
Background: Saliva is easily obtainable non-invasively and potentially suitable for detecting both current and previous SARS-CoV-2 infection, but there is limited evidence on the utility of salivary antibody testing for community surveillance.
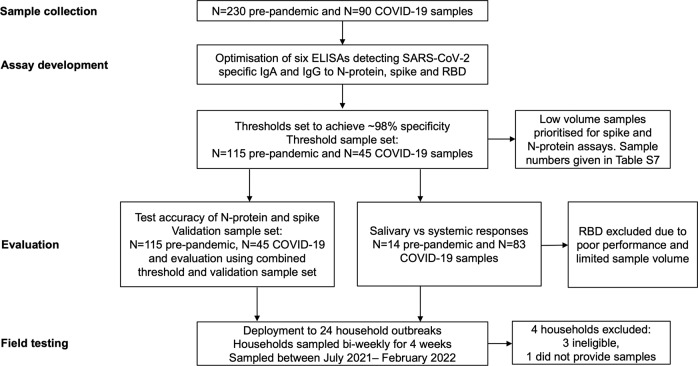
Methods: We established 6 ELISAs detecting IgA and IgG antibodies to whole SARS-CoV-2 spike protein, to its receptor binding domain region and to nucleocapsid protein in saliva. We evaluated diagnostic performance, and using paired saliva and serum samples, correlated mucosal and systemic antibody responses. The best-performing assays were field-tested in 20 household outbreaks.
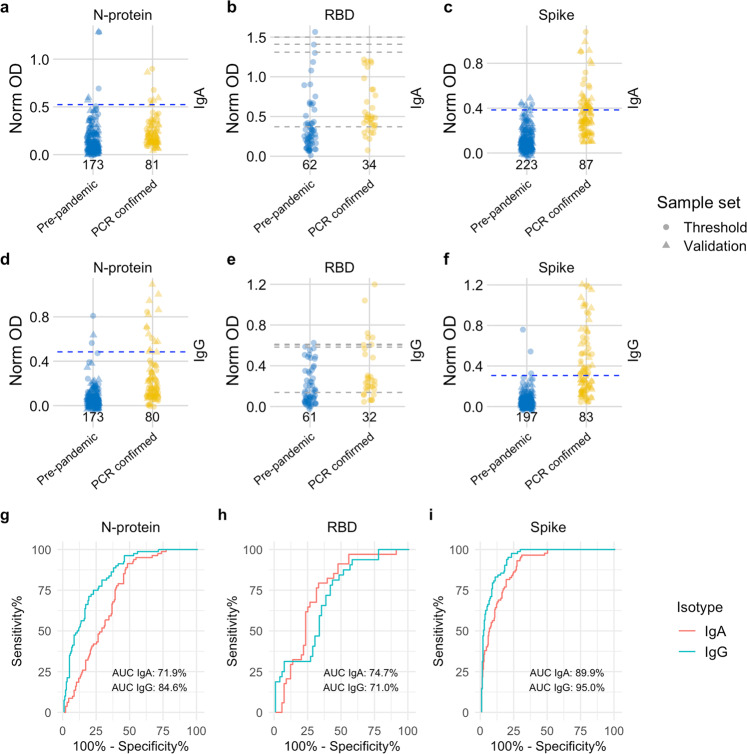
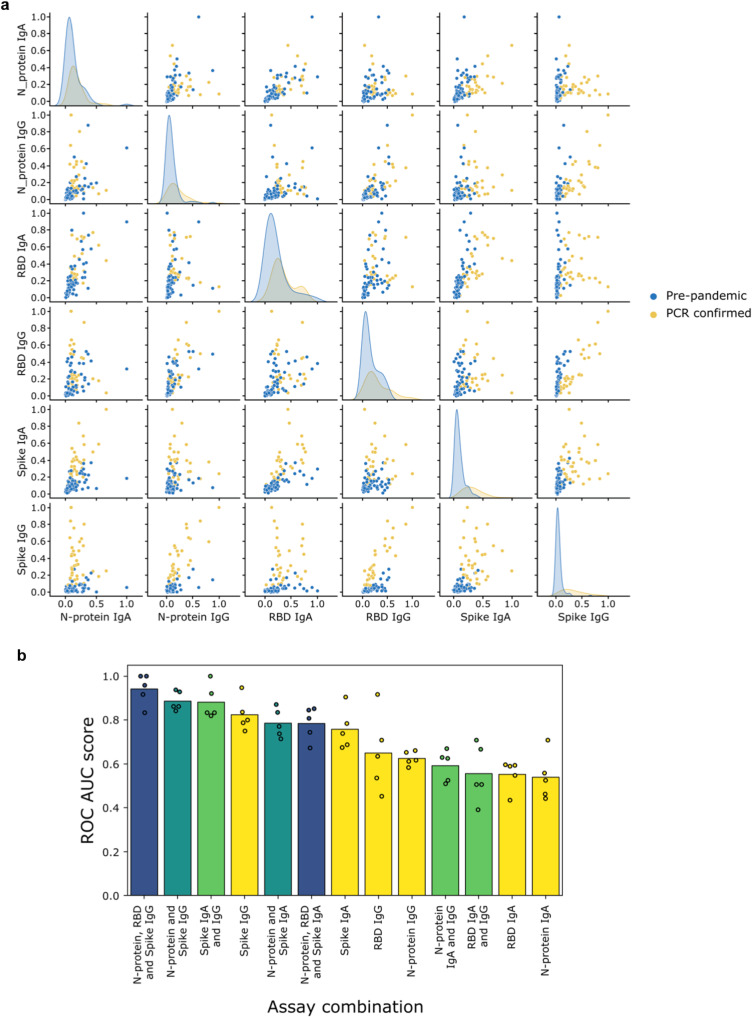
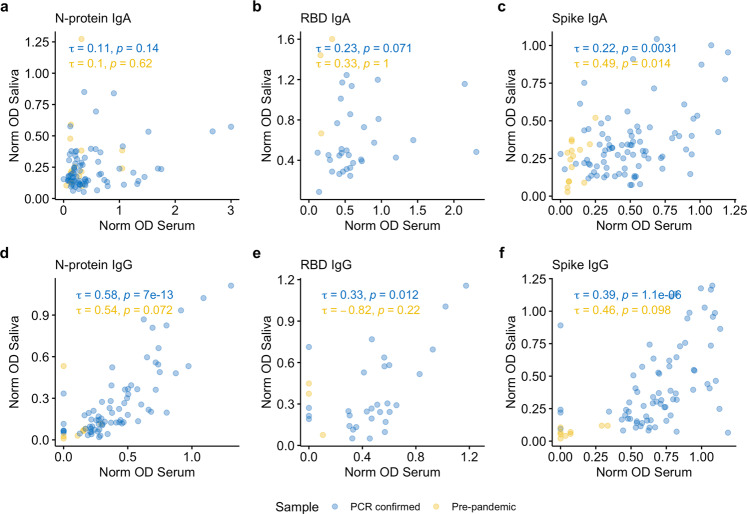
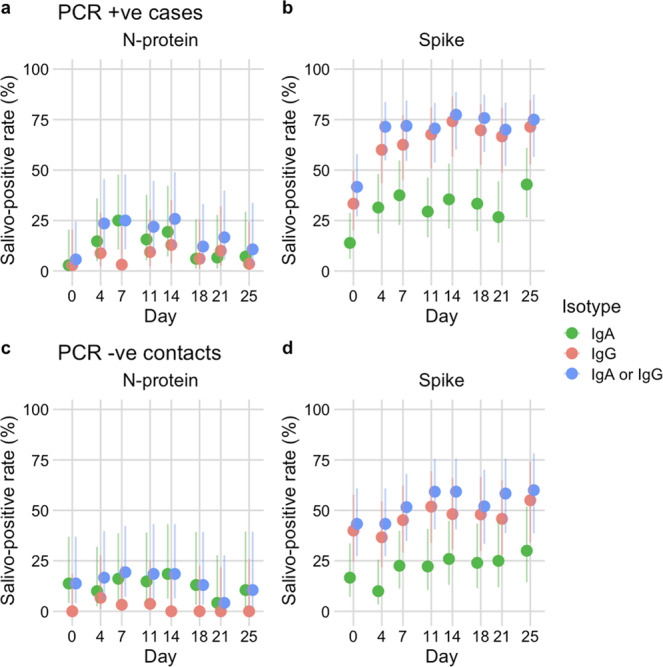
Results: We demonstrate in test accuracy (N = 320), spike IgG (ROC AUC: 95.0%, 92.8-97.3%) and spike IgA (ROC AUC: 89.9%, 86.5-93.2%) assays to discriminate best between pre-pandemic and post COVID-19 saliva samples. Specificity was 100% in younger age groups (0-19 years) for spike IgA and IgG. However, sensitivity was low for the best-performing assay (spike IgG: 50.6%, 39.8-61.4%). Using machine learning, diagnostic performance was improved when a combination of tests was used. As expected, salivary IgA was poorly correlated with serum, indicating an oral mucosal response whereas salivary IgG responses were predictive of those in serum. When deployed to household outbreaks, antibody responses were heterogeneous but remained a reliable indicator of recent infection. Intriguingly, unvaccinated children without confirmed infection showed evidence of exposure almost exclusively through specific IgA responses.
Conclusions: Through robust standardisation, evaluation and field-testing, this work provides a platform for further studies investigating SARS-CoV-2 transmission and mucosal immunity with the potential for expanding salivo-surveillance to other respiratory infections in hard-to-reach settings.
Plain language summary
If a person has been previously infected with SARS-CoV-2 they will produce specific proteins, called antibodies. These are present in the saliva and blood. Saliva is easier to obtain than blood, so we developed and evaluated six tests that detect SARS-CoV-2 antibodies in saliva in children and adults. Some tests detected antibodies to a particular protein made by SARS-CoV-2 called the spike protein, and these tests worked best. The most accurate results were obtained by using a combination of tests. Similar tests could also be developed to detect other respiratory infections which will enable easier identification of infected individuals.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: AF is a member of the Joint Committee on Vaccination and Immunisation, the UK national immunisation technical advisory group and is chair of the WHO European regional technical advisory group of experts (ETAGE) on immunisation and
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
