

The menin inhibitor revumenib in KMT2A-rearranged or NPM1-mutant leukaemia
- PMID: 36922593
- PMCID: PMC10060155
- DOI: 10.1038/s41586-023-05812-3
The menin inhibitor revumenib in KMT2A-rearranged or NPM1-mutant leukaemia
Abstract
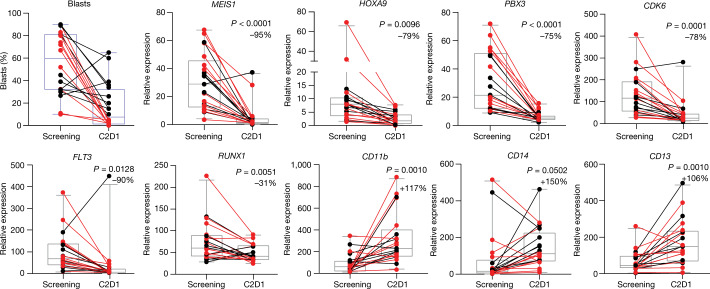
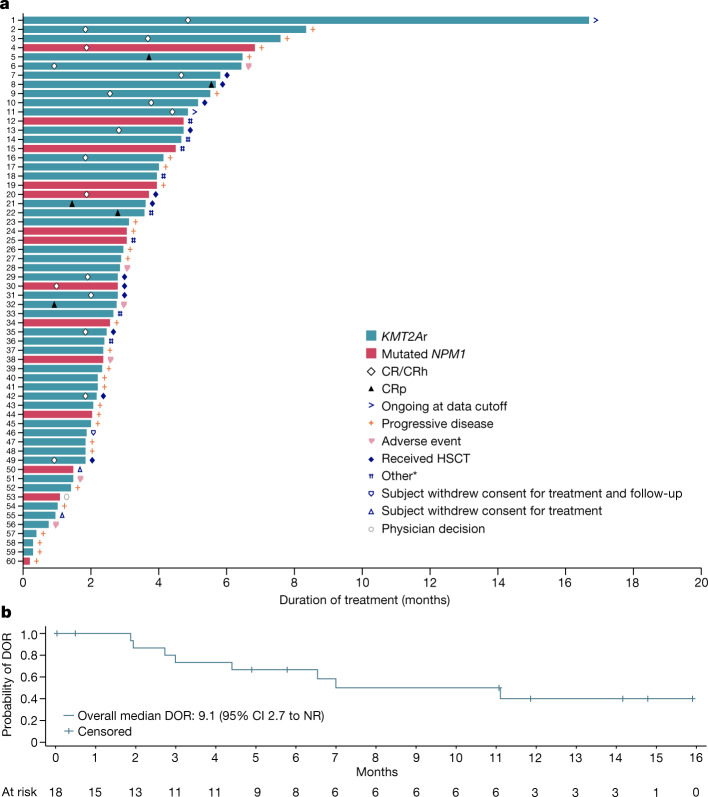
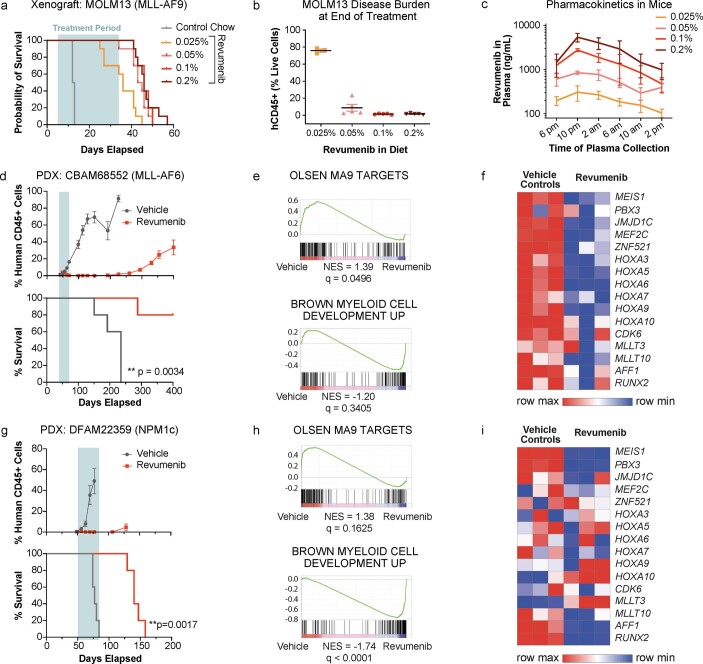
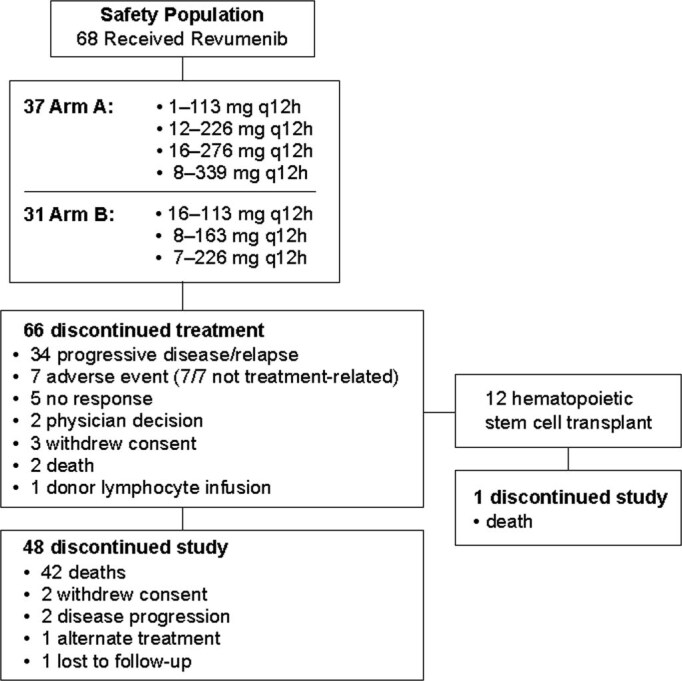
Targeting critical epigenetic regulators reverses aberrant transcription in cancer, thereby restoring normal tissue function1-3. The interaction of menin with lysine methyltransferase 2A (KMT2A), an epigenetic regulator, is a dependence in acute leukaemia caused by either rearrangement of KMT2A or mutation of the nucleophosmin 1 gene (NPM1)4-6. KMT2A rearrangements occur in up to 10% of acute leukaemias and have an adverse prognosis, whereas NPM1 mutations occur in up to 30%, forming the most common genetic alteration in acute myeloid leukaemia7,8. Here, we describe the results of the first-in-human phase 1 clinical trial investigating revumenib (SNDX-5613), a potent and selective oral inhibitor of the menin-KMT2A interaction, in patients with relapsed or refractory acute leukaemia (ClinicalTrials.gov, NCT04065399). We show that therapy with revumenib was associated with a low frequency of grade 3 or higher treatment-related adverse events and a 30% rate of complete remission or complete remission with partial haematologic recovery (CR/CRh) in the efficacy analysis population. Asymptomatic prolongation of the QT interval on electrocardiography was identified as the only dose-limiting toxicity. Remissions occurred in leukaemias refractory to multiple previous lines of therapy. We demonstrate clearance of residual disease using sensitive clinical assays and identify hallmarks of differentiation into normal haematopoietic cells, including differentiation syndrome. These data establish menin inhibition as a therapeutic strategy for susceptible acute leukaemia subtypes.
© 2023. The Author(s).
Conflict of interest statement
G.C.I. received consultancy or advisory role fees from Novartis, Kura Oncology and NuProbe and received research funding from Celgene, Novartis, Kura Oncology, Syndax Pharmaceuticals, Merck, Cullinan Oncology and NuProbe. I.A. received consultancy or advisory role fees from Amgen, Pfizer, Jazz, AbbVie and Agios, research funding from AbbVie and Macrogenics and honoraria from Amgen, Pfizer, Jazz, AbbVie and Agios. J.D.P. has a consultancy role with Incyte and RiverVest Venture Partners, has served as a board member or advisory committee member for RiverVest Venture Partners, Magenta, hC Bioscience, Inc. and WUGEN, has received research funding from NeoImmune Tech, Macrogenics, Incyte, Bioline Rx and WUGEN and holds patents or pending patents for UCART7 for treatment of T-ALL, VLA-4 inhibitors for stem cell mobilization and NT-I7 for CART expansion. R.S. has served on the steering committee of AbbVie and advisory boards of AbbVie, AvenCell, CTI Pharma, Kura One, Genentech, Actinium, Arog, BMS, Boston Pharmaceuticals, GSK, Janssen, Jazz, Novartis, Syros, Takeda, Elevate Bio, Syndax Pharmaceuticals, Gemoab, BerGenBio, Foghorn Tera, Aprea, Innate, Actinium and OncoNova; served as DSMB for Aptevo, Epizyme, Takeda and Syntrix/ACI Clinical; on the focus group of BerGenBio; and on AML Expert Council of GSK and Grand Rounds of Jazz Pharmaceuticals. M.A. has served on the advisory boards of Kite Pharma and Syndax Pharmaceuticals. M.J.T. has a consulting or advisory role with AbbVie and CVS, has an expert testimony role with Apotex and received research funding from AbbVie, Gilead Sciences, Janssen, Merck, Pharmacyclics, Syndax Pharmaceuticals, TG Therapeutics and Tolero. M.R.P. served in a leadership role with ION Pharma; received honoraria from Pfizer, Pharmacyclics, Bayer, Janssen Oncology, Genentech and Adaptive Biotechnologies; has a consulting or advisory role with Pharmacyclics/Janssen and Pfizer/EMD Serono; served on the Speakers’ Bureau of Exelixis, Genentech/Roche, Taiho Pharmaceutical and Celgene; and received research funding from Acerta Pharma, ADC Therapeutics, Agenus, Aileron Therapeutics, AstraZeneca, BioNTech AG, Boehringer Ingelheim, Celgene, Checkpoint Therapeutics, CicloMed, Clovis Oncology, Cyteir Therapeutics, Daiichi Sankyo, Lilly, EMD Serono, Evelo Therapeutics, FORMA Therapeutics, Genentech/Roche, Gilead Sciences, GlaxoSmithKline, H3 Biomedicine, Hengrui Therapeutics, Hutchison MediPharma, Ignyta, Incyte, Jacobio, Janssen, Klus Pharma, Kymab, Loxo, LSK Biopartners, Lycera, Macrogenics, Merck, Millennium, Mirati Therapeutics, Moderna Therapeutics, Pfizer, Placon, Portola Pharmaceuticals, Prelude Therapeutics, Ribon Therapeutics, Seven and Eight Biopharmaceuticals, Syndax Pharmaceuticals, Taiho Pharmaceutical, Takeda, Tesaro, TopAlliance BioSciences, Inc., Vigeo, ORIC, Artios, IgM Biosciences, Puretech, BioTheryX, Black Diamond Therapeutics, IgM Biosciences, NGM Biopharmaceuticals, Nurix, PureTech, Relay Therapeutics, Samumed, Silicon Therapeutics, TeneoBio, Treadwell Therapeutics, Zymeworks, Olema, Adagene, Astellas, NGM, Accutar Biotech, TeneoBio, Novartis, Compugen, Black Diamond Therapeutics, MabSpace Biosciences, Immunogen and Blueprint Pharmaceuticals. D.S.D. has a consulting or advisory role with Tempus, Inc. S. Shenoy has a consulting or advisory role with Artio, BMS and Takaeda. H.K. received honoraria/advisory board/consulting fees from AbbVie, Amgen, Amphista, Ascentage, Astellas, Biologix, Curis, Ipsen Biopharmaceuticals, KAHR Medical, Labcorp, Novartis, Pfizer, Shenzhen Target Rx, Stemline and Takeda; and received research funding from AbbVie, Amgen, Ascentage, BMS, Daiichi Sankyo, Immunogen, Jazz, and Novartis. S.A.A. received stock or other ownership from Neomorph, Inc., C4 Therapeutics, Cyteir Therapeutics, Accent Therapeutics and Mana Therapeutics; has a consulting or advisory role with Neomorph, Inc., C4 Therapeutics, Cyteir Therapeutics, Accent Therapeutics, Mana Therapeutics and Twentyeight-Seven Therapeutics; received research funding from Syndax Pharmaceuticals and Janssen; and holds patents, royalties and other intellectual property for MENIN inhibition in NPM1 AML: WO/2017/132398A1. G.R. is a former employee of Syndax Pharmaceuticals and a current employee of Boston Pharmaceuticals. R.G.B. is an employee of Syndax Pharmaceuticals and has stock or other ownership at Syndax Pharmaceuticals. M.L.M., P.O. and G.M.M. are employees of Syndax Pharmaceuticals. M.L.M. has a consulting or advisory role at Nuvalent, holds patents, royalties and other intellectual property at Syndax Pharmaceuticals and Nuvalent and has stock or other ownership at Syndax Pharmaceuticals and Johnson & Johnson. P.O. has a consulting or advisory role at Patrys and Twentyeight-Seven Therapeutics, holds patents, royalties and other intellectual property at Syndax Pharmaceuticals and has stock or other ownership at Syndax Pharmaceuticals. G.M.M. has a consulting or advisory role at Syndax Pharmaceuticals, holds patents, royalties and other intellectual property at Syndax Pharmaceuticals and has stock or other ownership at Syndax Pharmaceuticals. Y.G. is an employee of Syndax Pharmaceuticals and has stock or other ownership at Syndax Pharmaceuticals and AstraZeneca. S. Smith has a consultancy or advisory role with Syndax Pharmaceuticals. E.M.S. has a consulting or advisory role with Gilead, CTI Biopharma, Epizyme, AbbVie, Pinotbio, Neoleukin Genesis, Genentech, Jazz, Novartis, Celgene, Calithera, Takeda, Janssen, BMS, Kronos, Kura, Auron, Syndax Pharmaceuticals, Servier, Agios and Remix and received research funding from Biotheryx, Agios, Servier, Eisai, BMS, Bayer, Syndax, Syros and Loxo. B.C., F.P., J.A.P., N.S. and V.K. declare no competing interests.
Figures
Comment in
-
Investigating menin inhibitor action in leukaemia.Nat Rev Drug Discov. 2023 May;22(5):352. doi: 10.1038/d41573-023-00055-3. Nat Rev Drug Discov. 2023. PMID: 37016125 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
