

Lifetime impact of achondroplasia study in Europe (LIAISE): findings from a multinational observational study
- PMID: 36922864
- PMCID: PMC10015810
- DOI: 10.1186/s13023-023-02652-2
Lifetime impact of achondroplasia study in Europe (LIAISE): findings from a multinational observational study
Abstract
Background: Achondroplasia, caused by a pathogenic variant in the fibroblast growth factor receptor 3 gene, is the most common skeletal dysplasia. The Lifetime Impact of Achondroplasia Study in Europe (LIAISE; NCT03449368) aimed to quantify the burden of achondroplasia among individuals across a broad range of ages, including adults.
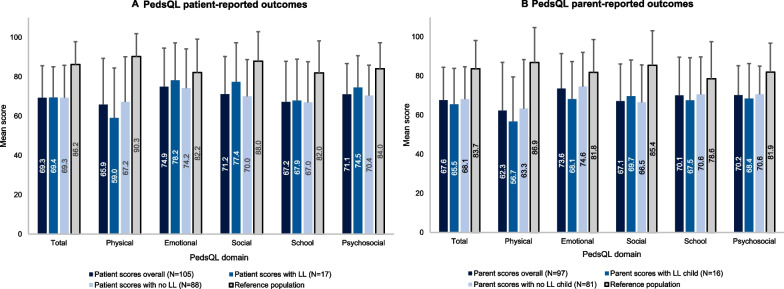
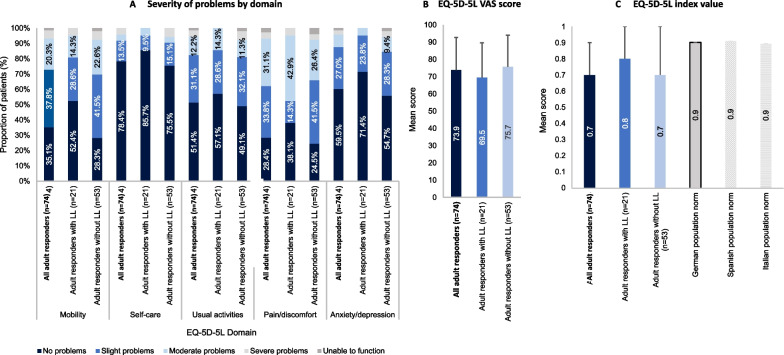
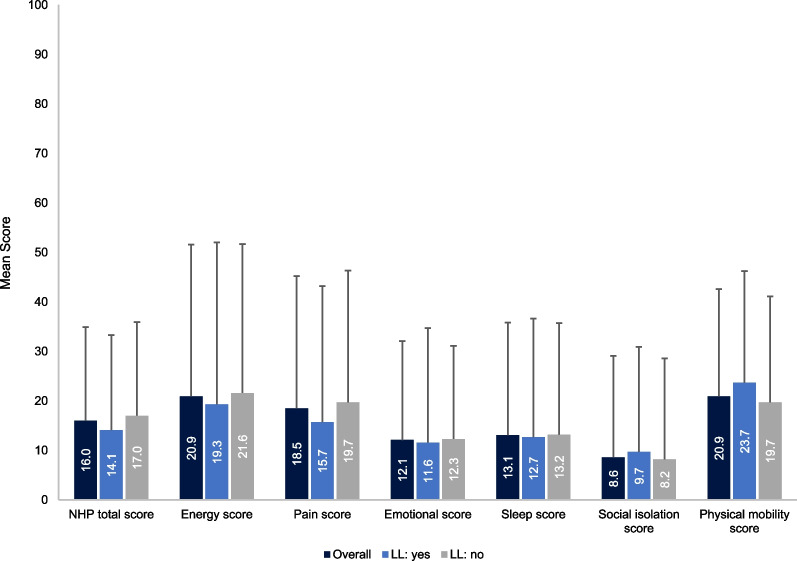
Methods: Demographic, clinical and healthcare resource use data were collected from medical records of achondroplasia patients enrolled in 13 sites across six European countries in this retrospective, observational study. Descriptive statistics or event rates per 100 person-years were calculated and compared across age groups as well as by history of limb lengthening. Patient-reported outcomes (quality of life [QoL], pain, functional independence, work productivity and activity impairments) were evaluated using questionnaires at the time of enrolment. An exploratory analysis investigated correlations between height (z-score or centimetres) and patient-reported outcomes.
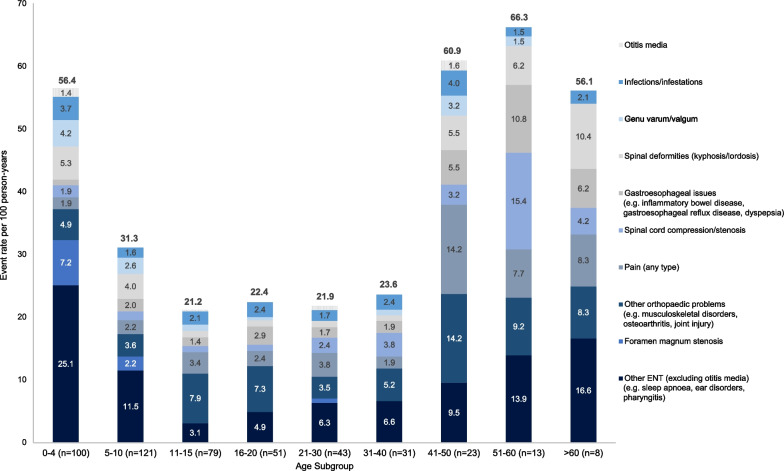
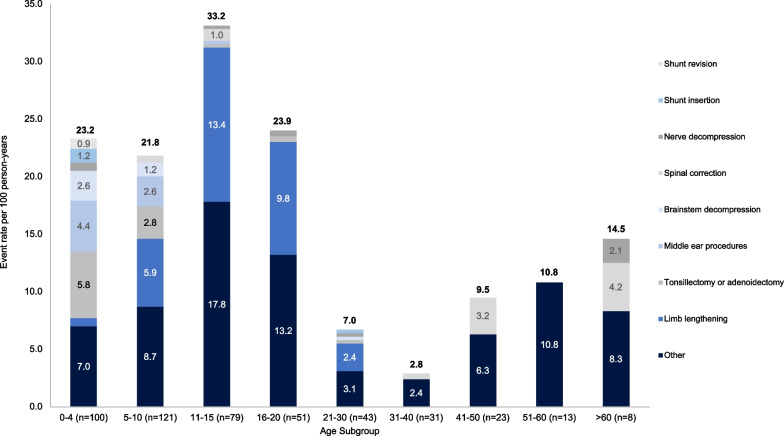
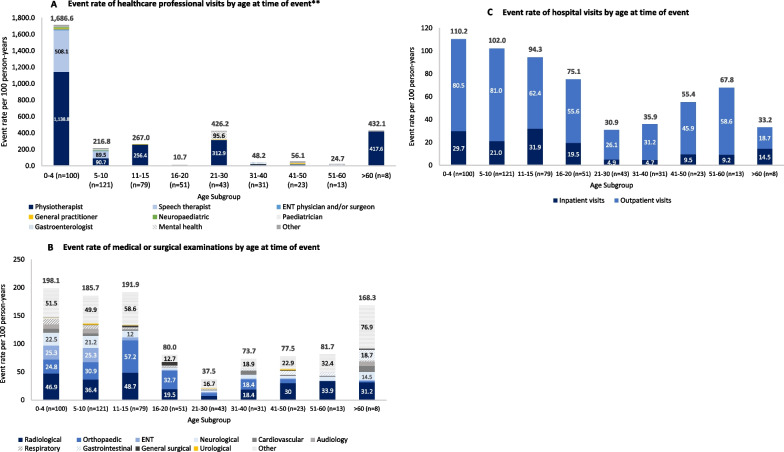
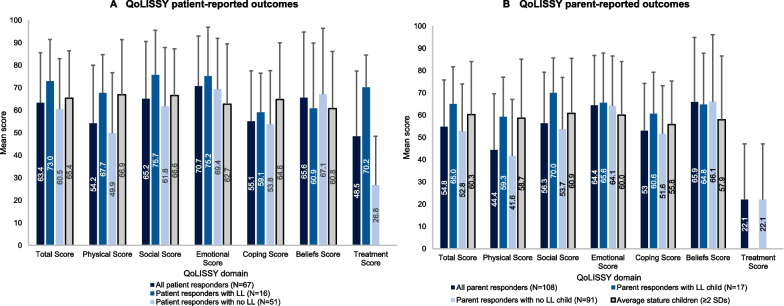
Results: Overall, 186 study patients were included, with a mean age of 21.7 ± 17.3 years (range 5.0-84.4). At least one complication or surgery was reported for 94.6% and 72.0% of patients, respectively, at a rate of 66.6 and 21.5 events per 100 person-years. Diverse medical and surgical complications were reported for all ages in a bimodal distribution, occurring more frequently in the youngest and oldest age groups. A total of 40 patients had previously undergone limb lengthening (capped at 20% per the study protocol). The most frequent surgery types varied by age, in line with complication profiles. Healthcare resource use was high across all age groups, especially among the youngest and oldest individuals, and did not differ substantially according to history of limb lengthening. Compared to general population values, patients reported impaired QoL particularly for physical functioning domains. In addition, patients reported difficulty carrying out daily activities independently and pain starting in childhood. Patient height correlated with multiple patient-reported outcomes.
Conclusions: The findings of this study suggest that, across an individual's lifetime, achondroplasia is associated with multisystem complications, reduced QoL and functionality, and increased pain. These results highlight the large amount of healthcare resources that individuals with achondroplasia require throughout their lifespans and provide novel insights into current achondroplasia management practices across Europe. Trial registration ClinicalTrials.gov, NCT03449368, Submitted 14 December 2017 - prospectively registered, https://clinicaltrials.gov/ct2/show/record/NCT03449368.
Keywords: Achondroplasia; Disease burden; Fibroblast growth factor receptor 3 (FGFR3); Natural history; Skeletal dysplasia.
© 2023. The Author(s).
Conflict of interest statement
MM: Grant support from Pfizer, Novo Nordisk and Merck Serono and consultancy honoraria and speaker fees from Merck Serono, Novo Nordisk, Pfizer, Sandoz, and BioMarin. OS: Speaker fees from BioMarin. EGN: Has received research support, consultation fees and travel support from BioMarin. AS: Consultancy honoraria from BioMarin. KEH: No conflicts of interest in the context of the current study. GH: No conflicts of interest in the context of the current study. LH: Research grants from Pfizer and BioMarin; consultant and lecture fees from Novo Nordisk and Sanofi. AM: No conflicts of interest in the context of the current study. ALG: ALG and Orthopedic and Trauma Research Group (FA-07), IBIMA Tech Unit, has received fees relationship with clinical trials development by BioMarin and QED Therapeutics. These fees do not pose a conflict of interest in connection with the submitted article. VLG: No conflicts of interest in the context of the current study. AR: No conflicts of interest in the context of the current study. MR: No conflicts of interest in the context of the current study. FSS: Advisory consultation fees from BioMarin. DAE: No conflicts of interest in the context of the current study. PAG: BioMarin honoraria for Steering Committee participation. RO: No conflicts of interest in the context of the current study. EL: No conflicts of interest in the context of the current study. JJ: At the time of the research, JJ was a full time employee of BioMarin and held stocks in the company. JQ: At the time of the research, JJ was a full time employee of BioMarin and held stocks in the company. RR, RS, SC, JMP, TB, SM: Full time employees of BioMarin and hold stocks in the company. KM: Honoraria by BioMarin and QED.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
