

Association of COVID-19 with Comorbidities: An Update
- PMID: 36923110
- PMCID: PMC10000013
- DOI: 10.1021/acsptsci.2c00181
Association of COVID-19 with Comorbidities: An Update
Abstract
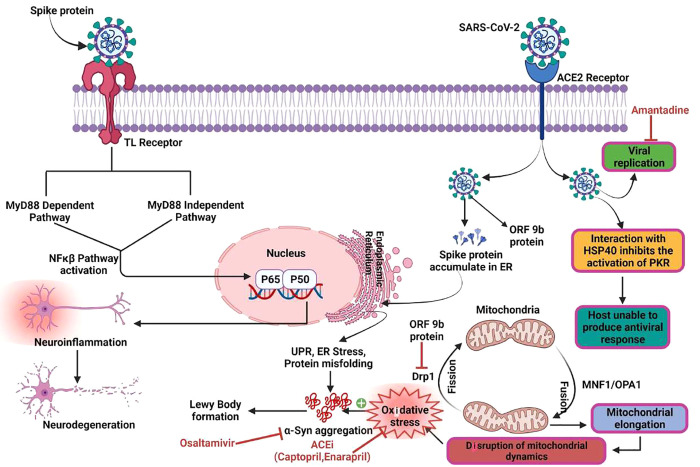
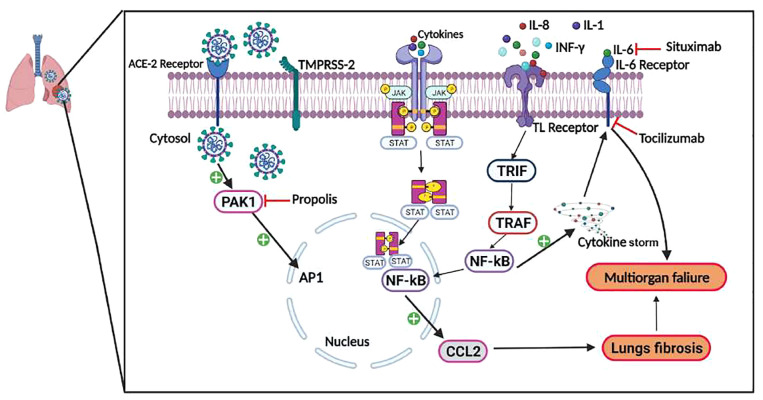
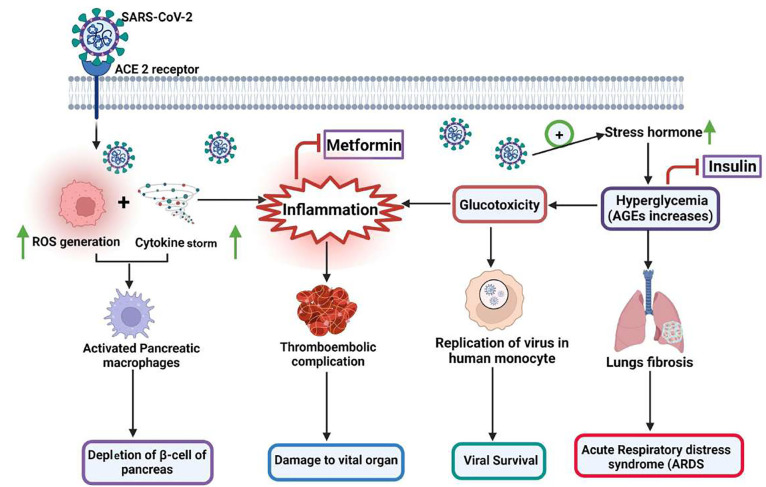
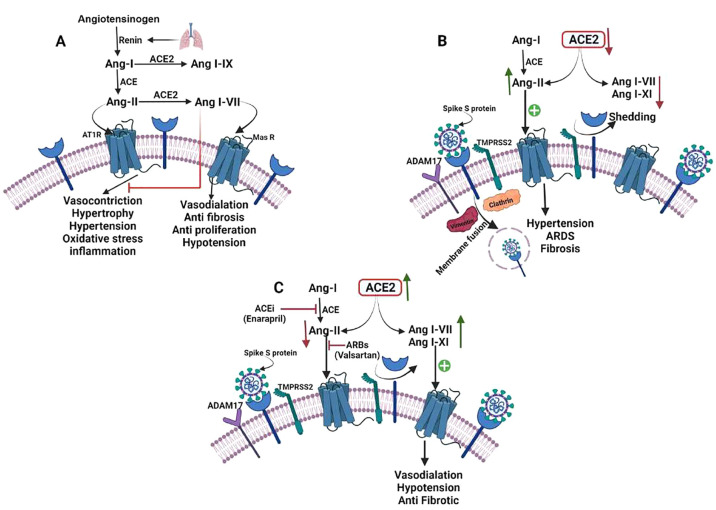
Coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) which was identified in Wuhan, China in December 2019 and jeopardized human lives. It spreads at an unprecedented rate worldwide, with serious and still-unfolding health conditions and economic ramifications. Based on the clinical investigations, the severity of COVID-19 appears to be highly variable, ranging from mild to severe infections including the death of an infected individual. To add to this, patients with comorbid conditions such as age or concomitant illnesses are significant predictors of the disease's severity and progression. SARS-CoV-2 enters inside the host cells through ACE2 (angiotensin converting enzyme2) receptor expression; therefore, comorbidities associated with higher ACE2 expression may enhance the virus entry and the severity of COVID-19 infection. It has already been recognized that age-related comorbidities such as Parkinson's disease, cancer, diabetes, and cardiovascular diseases may lead to life-threatening illnesses in COVID-19-infected patients. COVID-19 infection results in the excessive release of cytokines, called "cytokine storm", which causes the worsening of comorbid disease conditions. Different mechanisms of COVID-19 infections leading to intensive care unit (ICU) admissions or deaths have been hypothesized. This review provides insights into the relationship between various comorbidities and COVID-19 infection. We further discuss the potential pathophysiological correlation between COVID-19 disease and comorbidities with the medical interventions for comorbid patients. Toward the end, different therapeutic options have been discussed for COVID-19-infected comorbid patients.
© 2023 American Chemical Society.
Conflict of interest statement
The authors declare no competing financial interest.
Figures
References
-
- Coronavirus resources center.https://coronavirus.jhu.edu/ (acccessed 05–12–2022).
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous