

Effect of Suture Length on the Incidence of Incisional Hernia and Surgical Site Infection in Patients Undergoing Midline Laparotomy: A Systematic Review and Meta-Analysis
- PMID: 36923180
- PMCID: PMC10010319
- DOI: 10.7759/cureus.34840
Effect of Suture Length on the Incidence of Incisional Hernia and Surgical Site Infection in Patients Undergoing Midline Laparotomy: A Systematic Review and Meta-Analysis
Abstract
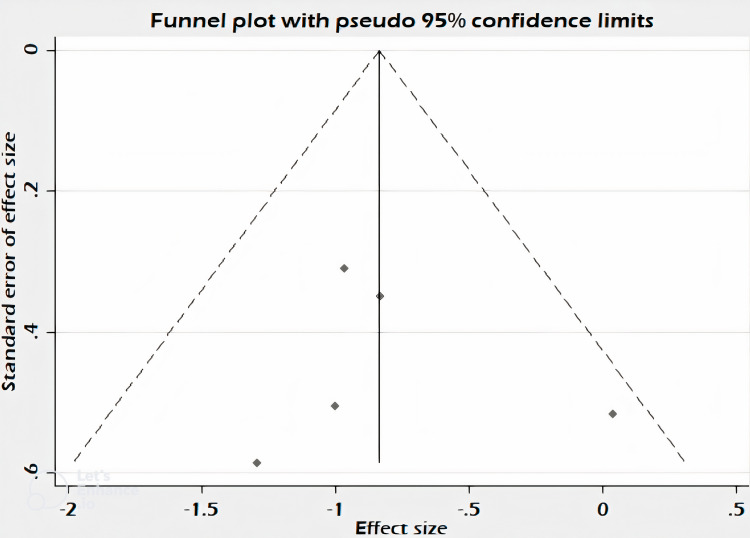
The development of an incisional hernia is a common complication of midline laparotomy. Improper fascial closure techniques have a significant role in its development. It can also lead to poor wound healing and increase the risk of developing surgical site infections (SSI). Upon conducting a thorough literature review, various studies have been conducted on closing abdominal wounds. However, there is a dearth of studies portraying the role of suture length in the prevention of incisional hernia and SSI. The effect of using a greater suture-to-wound length ratio on postoperative outcomes was not clearly analyzed or described. The objective of this study is to assess the effectiveness of using a suture length to wound length ratio ≥4:1 versus a ratio <4:1 in preventing postoperative complications such as incisional hernia and SSI. This study is a systematic review of randomized controlled trials on abdominal wound closure using a suture length to wound length ratio of ≥4:1 and <4:1. published in PubMed, Google Scholar, and Cochrane library. The inclusion and exclusion criteria were defined. The relevant studies identified from 1991 to 2017, were included in the analysis. The primary endpoint was the incidence of incisional hernia, and the secondary outcome was the incidence of SSI. This meta-analysis considered five randomized controlled trials that compared the effects of using different suture length to wound length ratios during abdominal closure on incisional hernia and SSI. Participants ranged in size from 100 to 363. The trial follow-up period ranged from a minimum of 10 months to five years. The outcomes studied in the two groups were incisional hernia and SSI. The relative risk of the occurrence of incisional hernia if the suture length to wound length ratio was ≥4:1 was 0.42 with a p-value of <0.001 which was considered significant. This implied that using a suture length of more than four times that of the wound i.e., 4:1, significantly decreases the risk of developing an incisional hernia by more than half. The relative risk of developing a SSI was 0.98 with a p-value of 0.966. Thus, this method of abdominal closure uing a longer suture length to wound length ratio does not contribute to an increased incidence or significant change in the risk of developing SSI.
Keywords: incidence; incisional hernia; midline laparotomy; ratio; surgical site infection; suture length; wound length.
Copyright © 2023, Sekhar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Incidence and prevention of ventral incisional hernia. Le Huu Nho R, Mege D, Ouaïssi M, Sielezneff I, Sastre B. J Visc Surg. 2012;149:0. - PubMed
-
- Classification and surgical treatment of incisional hernia. Results of an experts' meeting. Korenkov M, Paul A, Sauerland S, et al. Langenbecks Arch Surg. 2001;386:65–73. - PubMed
-
- Incidence and risk factors for incisional hernia and recurrence: retrospective analysis of the French national database. Gignoux B, Bayon Y, Martin D, Phan R, Augusto V, Darnis B, Sarazin M. Colorectal Dis. 2021;23:1515–1523. - PubMed
-
- The burst abdominal wound: a mechanical approach. Jenkins TP. Br J Surg. 1976;63:873–876. - PubMed
Publication types
LinkOut - more resources
Full Text Sources