

Preoperative ultrasound identification and localization of the inferior parathyroid glands in thyroid surgery
- PMID: 36923217
- PMCID: PMC10009105
- DOI: 10.3389/fendo.2023.1094379
Preoperative ultrasound identification and localization of the inferior parathyroid glands in thyroid surgery
Abstract
Introduction: The parathyroid glands are important endocrine glands for maintaining calcium and phosphorus metabolism, and they are vulnerable to accidental injuries during thyroid cancer surgery. The aim of this retrospective study was to investigate the application of high-frequency ultrasound imaging for preoperative anatomical localization of the parathyroid glands in patients with thyroid cancer and to analyze the protective effect of this technique on the parathyroid glands and its effect on reducing postoperative complications.
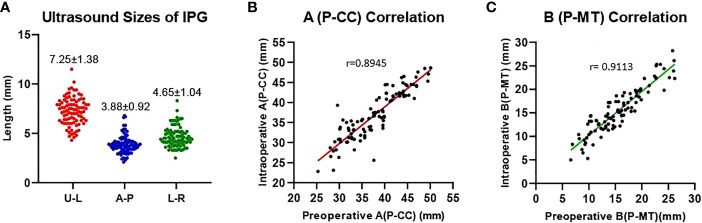
Materials and methods: A total of 165 patients who were operated for thyroid cancer in our hospital were included. The patients were assigned into two groups according to the time period of surgery: Control group, May 2018 to February 2021 (before the application of ultrasound localization of parathyroid in our hospital); PUS group, March 2021 to May 2022. In PUS group, preoperative ultrasound was used to determine the size and location of bilateral inferior parathyroid glands to help surgeons identify and protect the parathyroid glands during operation. We compared the preoperative ultrasound results with the intraoperative observations. Preoperative and first day postoperative serum calcium and PTH were measured in both groups.
Results: Our preoperative parathyroid ultrasound identification technique has more than 90% accuracy (true positive rate) to confirm the location of parathyroid gland compared to intraoperative observations. Postoperative biochemical results showed a better Ca2+ [2.12(0.17) vs. 2.05(0.31), P=0.03] and PTH [27.48(14.88) vs. 23.27(16.58), P=0.005] levels at first day post-operation in PUS group compared to control group. We also found a reduced risk of at least one type of hypoparathyroidism after surgery in control group:26 cases (31.0%) vs. 41 cases (50.6%), p=0.016.
Conclusion: Ultrasound localization of the parathyroid glands can help in the localization, identification and in situ preservation of the parathyroid glands during thyroidectomy. It can effectively reduce the risk of hypoparathyroidism after thyroid surgery.
Keywords: clinical effect; hypoparathyroidism; parathyroid gland; thyroid cancer; ultrasound localization.
Copyright © 2023 Chen, Zhang, Liu, Guo, Liu and Geng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous