

Protective potential of the gallbladder in primary sclerosing cholangitis
- PMID: 36923239
- PMCID: PMC10009728
- DOI: 10.1016/j.jhepr.2022.100649
Protective potential of the gallbladder in primary sclerosing cholangitis
Abstract
Background & aims: Gallbladder enlargement is common in patients with primary sclerosing cholangitis (PSC). The gallbladder may confer hepatoprotection against bile acid overload, through the sequestration and cholecystohepatic shunt of bile acids. The aim of this study was to assess the potential impact of the gallbladder on disease features and bile acid homeostasis in PSC.
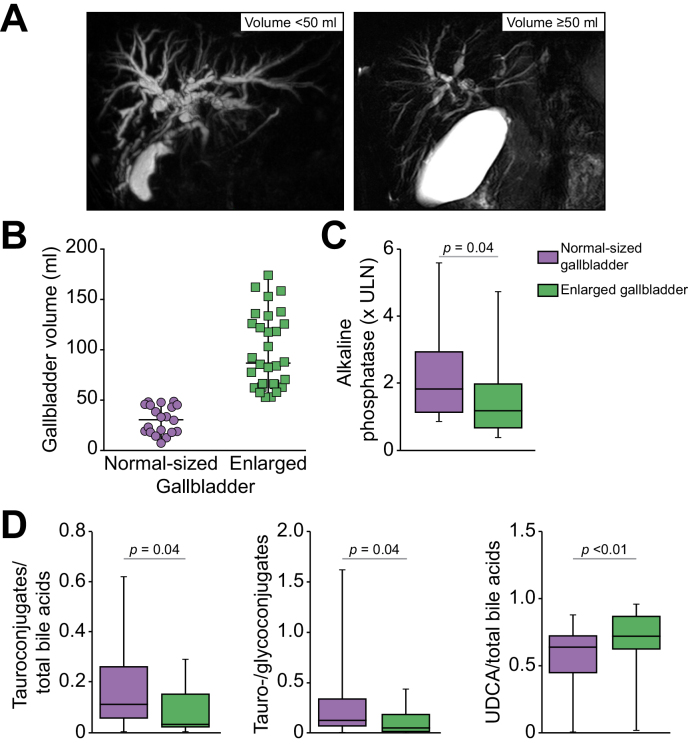
Methods: Patients with PSC from a single tertiary center who underwent liver MRI with three-dimensional cholangiography and concomitant analyses of serum bile acids were included. Gallbladder volume was measured by MRI and a cut-off of 50 ml was used to define gallbladder enlargement. Bile acid profiles and PSC severity, as assessed by blood tests and MRI features, were compared among patients according to gallbladder size (enlarged vs. normal-sized) or presence (removed vs. conserved). The impact of cholecystectomy was also assessed in the Abcb4 knockout mouse model of PSC.
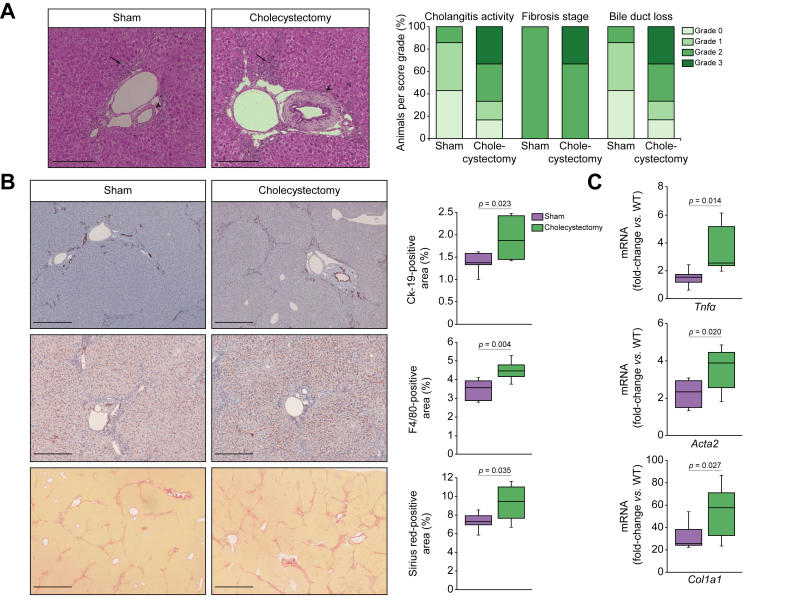
Results: Sixty-one patients with PSC, all treated with ursodeoxycholic acid (UDCA), were included. The gallbladder was enlarged in 30 patients, whereas 11 patients had been previously cholecystectomized. Patients with enlarged gallbladders had significantly lower alkaline phosphatase, a lower tauro-vs. glycoconjugate ratio and a higher UDCA vs. total bile acid ratio compared to those with normal-sized gallbladders. In addition, gallbladder volume negatively correlated with the hydrophobicity index of bile acids. Cholecystectomized patients displayed significantly higher aspartate aminotransferase and more severe bile duct strictures and dilatations compared to those with conserved gallbladder. In the Abcb4 knockout mice, cholecystectomy caused an increase in hepatic bile acid content and in circulating secondary bile acids, and an aggravation in cholangitis, inflammation and liver fibrosis.
Conclusion: Altogether, our findings indicate that the gallbladder fulfills protective functions in PSC.
Impact and implications: In patients with primary sclerosing cholangitis (PSC), gallbladder status impacts on bile acid homeostasis and disease features. We found evidence of lessened bile acid toxicity in patients with PSC and enlarged gallbladders and of increased disease severity in those who were previously cholecystectomized. In the Abcb4 knockout mouse model of PSC, cholecystectomy causes an aggravation of cholangitis and liver fibrosis. Overall, our results suggest that the gallbladder plays a protective role in PSC.
Keywords: ABC, ATP-binding cassette transporter; Abcb4 knockout mice; BA, bile acid; Bile acids; C4, 7α-hydroxy-4-cholesten-3-one; CFTR, cystic fibrosis transmembrane conductance regulator; CK19, cytokeratin 19; Cholecystectomy; FGF19, fibroblast growth factor 19; Gallbladder volume; HPLC-MS/MS, high-performance liquid chromatography coupled to tandem mass spectrometry; IBD, inflammatory bowel disease; MRC, magnetic resonance cholangiography; Magnetic resonance imaging; PSC, primary sclerosing cholangitis; UDCA, ursodeoxycholic acid; ULN, upper limit of normal.
© 2022 The Authors.
Conflict of interest statement
Nora Cazzagon, Ester Gonzalez-Sanchez, Haquima El-Mourabit, Dominique Wendum, Dominique Rainteau, Lydie Humbert, Olivier Chazouillères, Lionel Arrivé, Chantal Housset and Sara Lemoinne declare no conflict of interest related to this paper. Christophe Corpechot declares the following conflicts of interest: Intercept, Arrow, Cymabay, Ipsen, Calliditas, Gilead. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
-
- Karlsen T.H., Folseraas T., Thorburn D., Vesterhus M. Primary sclerosing cholangitis - a comprehensive review. J Hepatol. 2017;67:1298–1323. - PubMed
-
- Boonstra K., Weersma R.K., van Erpecum K.J., Rauws E.A., Spanier B.W.M., Poen A.C., et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology. 2013;58:2045–2055. - PubMed
-
- Trivedi P.J., Crothers H., Mytton J., Bosch S., Iqbal T., Ferguson J., et al. Effects of primary sclerosing cholangitis on risks of cancer and death in people with inflammatory bowel disease, based on sex, race, and age. Gastroenterology. 2020;159:915–928. - PubMed
-
- Al Mamari S., Djordjevic J., Halliday J.S., Chapman R.W. Improvement of serum alkaline phosphatase to <1.5 upper limit of normal predicts better outcome and reduced risk of cholangiocarcinoma in primary sclerosing cholangitis. J Hepatol. 2013;58:329–334. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
