

Pathogen spectra in hospitalised and nonhospitalised children with community-acquired pneumonia
- PMID: 36923566
- PMCID: PMC10009707
- DOI: 10.1183/23120541.00286-2022
Pathogen spectra in hospitalised and nonhospitalised children with community-acquired pneumonia
Abstract
Background: Paediatric community-acquired pneumonia (CAP) is a leading cause of paediatric morbidity. However, particularly for outpatients with paediatric CAP, data on aetiology and management are scarce.
Methods: The prospective pedCAPNETZ study multicentrically enrols children and adolescents with outpatient-treated or hospitalised paediatric CAP in Germany. Blood and respiratory specimens were collected systematically, and comprehensive analyses of pathogen spectra were conducted. Follow-up evaluations were performed until day 90 after enrolment.
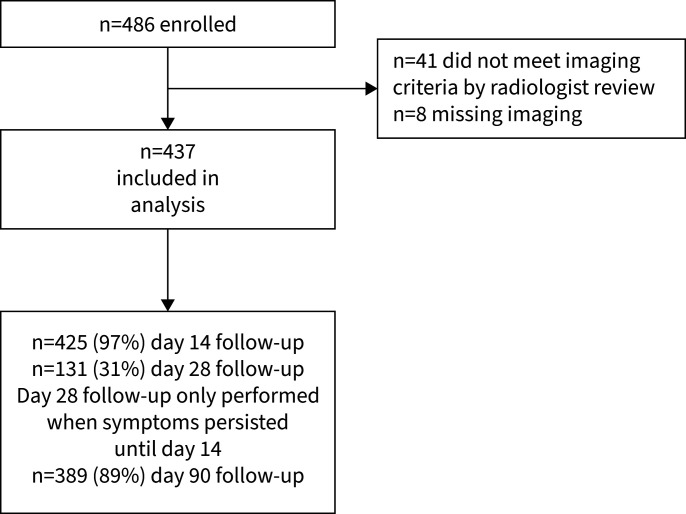
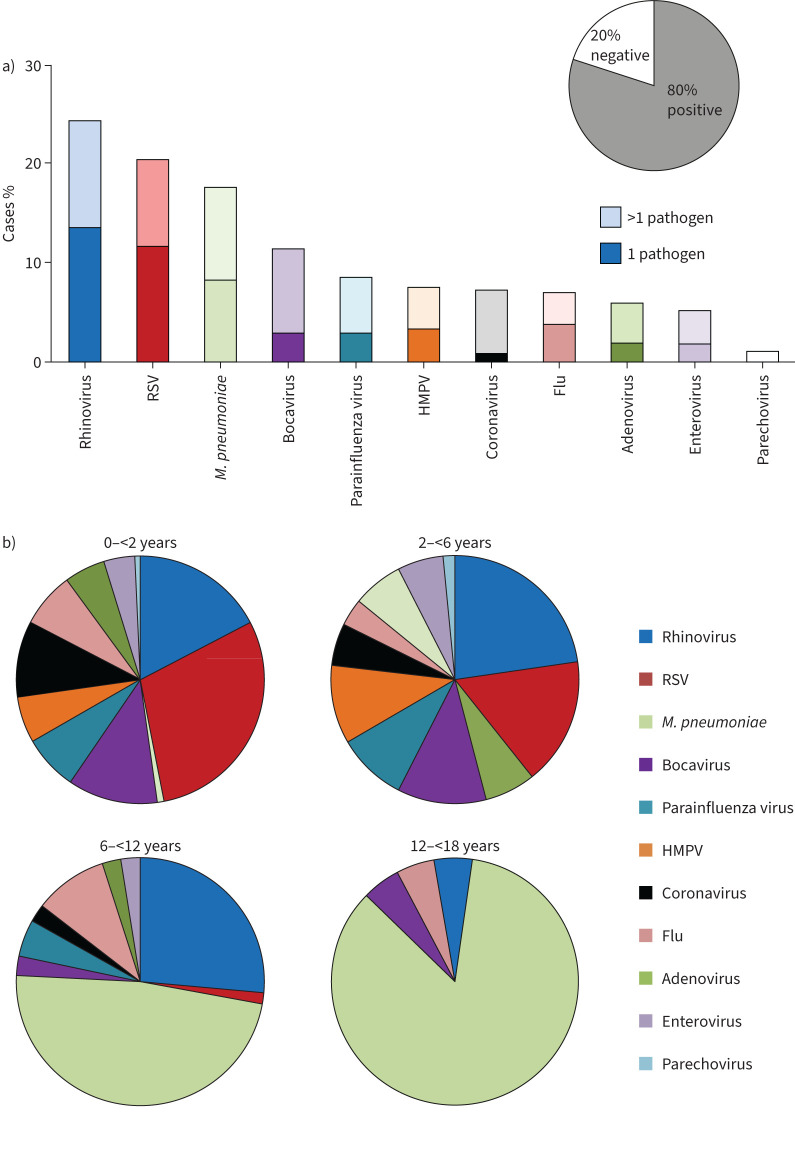
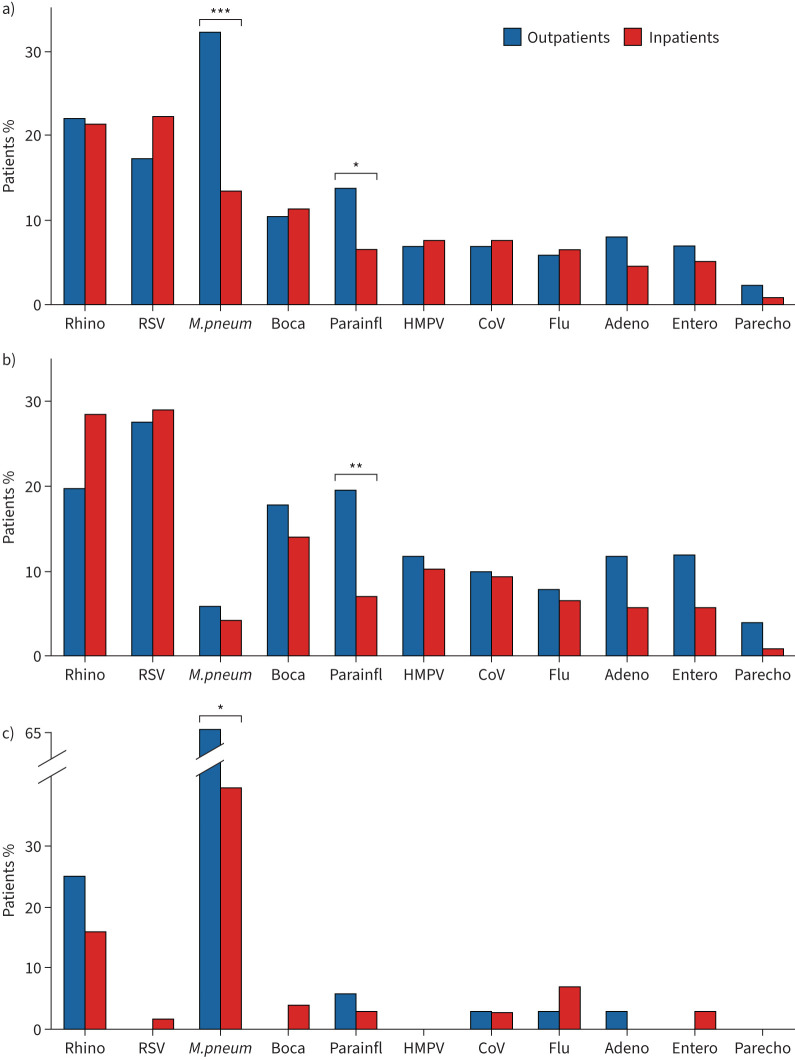
Results: Between December 2014 and August 2020, we enrolled 486 children with paediatric CAP at eight study sites, 437 (89.9%) of whom had radiographic evidence of paediatric CAP. Median (interquartile range) age was 4.5 (1.6-6.6) years, and 345 (78.9%) children were hospitalised. The most prevalent symptoms at enrolment were cough (91.8%), fever (89.2%) and tachypnoea (62.0%). Outpatients were significantly older, displayed significantly lower C-reactive protein levels and were significantly more likely to be symptom-free at follow-up days 14 and 90. Pathogens were detected in 90.3% of all patients (one or more viral pathogens in 68.1%; one or more bacterial strains in 18.7%; combined bacterial/viral pathogens in 4.1%). Parainfluenza virus and Mycoplasma pneumoniae were significantly more frequent in outpatients. The proportion of patients with antibiotic therapy was comparably high in both groups (92.4% of outpatients versus 86.2% of hospitalised patients).
Conclusion: We present first data on paediatric CAP with comprehensive analyses in outpatients and hospitalised cases and demonstrate high detection rates of viral pathogens in both groups. Particularly in young paediatric CAP patients with outpatient care, antibiotic therapy needs to be critically debated.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: M. Wetzke received funding from the Young Academy Clinician/Scientist foundation Hannover Medical School, Germany and the Clinical Leave Clinician/Scientist program of the German Center for Infection Research (DZIF). K. Schütz and G. Hansen received funding from the Deutsche Forschungsgemeinschaft for the Cluster of Excellence EXC2155 “RESIST” project (ID 39087428). C. Happle received funding from the Young Academy Clinician/Scientist foundation and HiLF funding of Hannover Medical School, Germany, and the Excellence Cluster RESIST in infection research. M.V. Kopp, G. Hansen and T. Welte received funding from the German Center for Lung Research (DZL). The other authors received no additional funding. The authors have no conflicts of interests for this article to disclose.
Figures
References
-
- Gesundheitsberichterstattung des Bundes . Diagnosedaten der Krankenhäuser ab 2000 [Hospital Diagnostic Data Since 2000]. https://www.gbe-bund.de/gbe/!pkg_olap_tables.prc_set_orientation?p_uid=g... Date last accessed: 14 December 2022.
-
- Pneumonia Etiology Research for Child Health (PERCH) Study Group. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet 2019; 394: 757–779. doi: 10.1016/S0140-6736(19)30721-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous