

Cardiac sarcoidosis: phenotypes, diagnosis, treatment, and prognosis
- PMID: 36924191
- PMCID: PMC10149532
- DOI: 10.1093/eurheartj/ehad067
Cardiac sarcoidosis: phenotypes, diagnosis, treatment, and prognosis
Abstract
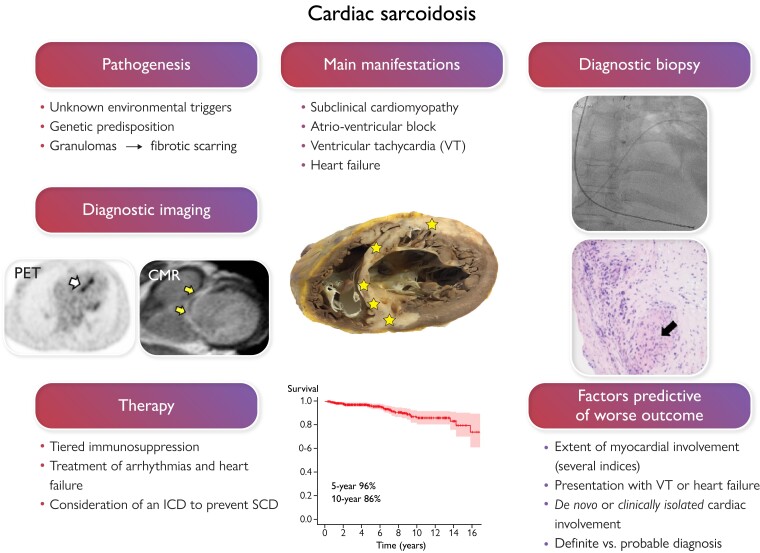
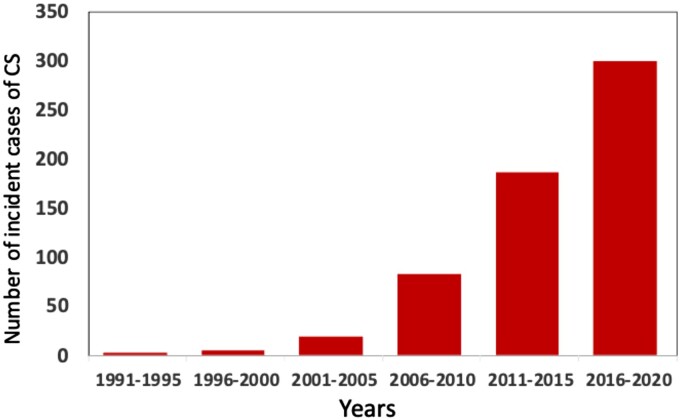
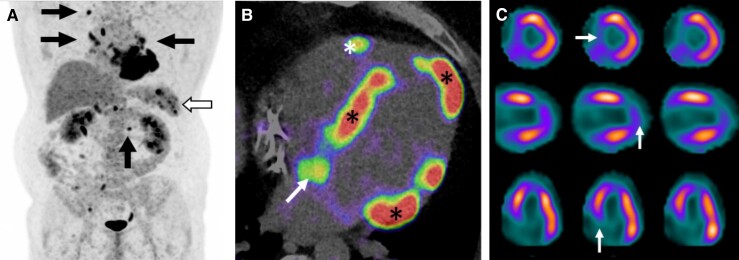
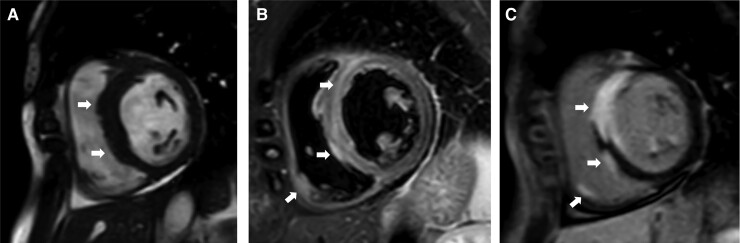
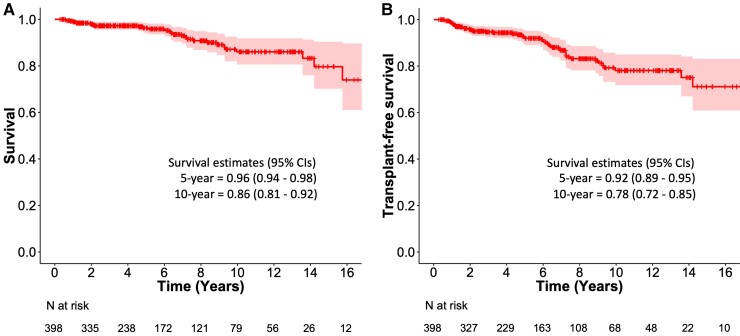
Cardiac sarcoidosis (CS) results from epithelioid cell granulomas infiltrating the myocardium and predisposing to conduction disturbances, ventricular tachyarrhythmias, and heart failure. Manifest CS, however, constitutes only the top of an iceberg as advanced imaging uncovers cardiac involvement 4 to 5 times more commonly than what is clinically detectable. Definite diagnosis of CS requires myocardial biopsy and histopathology, but a sufficient diagnostic likelihood can be achieved by combining extracardiac histology of sarcoidosis with clinical manifestations and findings on cardiac imaging. CS can appear as the first or only organ manifestation of sarcoidosis or on top of pre-existing extracardiac disease. Due to the lack of controlled trials, the care of CS is based on observational evidence of low quality. Currently, the treatment involves corticosteroid-based, tiered immunosuppression to control myocardial inflammation with medical and device-based therapy for symptomatic atrioventricular block, ventricular tachyarrhythmias, and heart failure. Recent outcome data indicate 90% to 96% 5-year survival in manifest CS with the 10-year figures ranging from 80% to 90%. Major progress in the care of CS awaits the key to its molecular-genetic pathogenesis and large-scale controlled clinical trials.
Keywords: Cardiac sarcoidosis; Heart failure; Implantable cardioverter-defibrillator; Inflammatory heart disease; Pacemaker.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest Lecture and/or advisory board fees from Boehringer Ingelheim, Bristol-Myers Squibb, MSD, Takeda, Bayer, Amgen, Roche, and Aiforia technologies oy (M.I.M.). Lecture fee from Pfizer and research collaboration with GE healthcare (V.U.).
Figures
References
-
- Drent M, Crouser ED, Grunewald J. Challenges of Sarcoidosis and Its Management. N Engl J Med 2021;385:1018–1032. - PubMed
-
- Kandolin R, Lehtonen J, Airaksinen J, Vihinen T, Miettinen H, Ylitalo K, et al. . Cardiac sarcoidosis: epidemiology, characteristics, and outcome over 25 years in a nationwide study. Circulation 2015;131:624–632. - PubMed
-
- Judson M, Costabel U, Drent Met al. . The WASOG Sarcoidosis Organ Assessment Instrument: an update of a previous clinical tool. Sarcoidosis Vasc Diffuse Lung Dis 2014;31:19–27. - PubMed
-
- Birnie DH, Sauer WH, Bogun F, Cooper JM, Culver DA, Duvernoy CS, et al. . HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm 2014;11:1305–1323. - PubMed
-
- Terasaki F, Azuma A, Anzai T, Ishizaka N, Ishida Y, Isobe M, et al. . Japanese Circulation Society Joint Working Group. JCS 2016 Guideline on Diagnosis and Treatment of Cardiac Sarcoidosis. Circ J 2019;83:2329–2388. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
