

Estimating national-level measles case-fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study
- PMID: 36925172
- PMCID: PMC10030458
- DOI: 10.1016/S2214-109X(23)00043-8
Estimating national-level measles case-fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study
Abstract
Background: To understand the current measles mortality burden, and to mitigate the future burden, it is crucial to have robust estimates of measles case fatalities. Estimates of measles case-fatality ratios (CFRs) that are specific to age, location, and time are essential to capture variations in underlying population-level factors, such as vaccination coverage and measles incidence, which contribute to increases or decreases in CFRs. In this study, we updated estimates of measles CFRs by expanding upon previous systematic reviews and implementing a meta-regression model. Our objective was to use all information available to estimate measles CFRs in low-income and middle-income countries (LMICs) by country, age, and year.
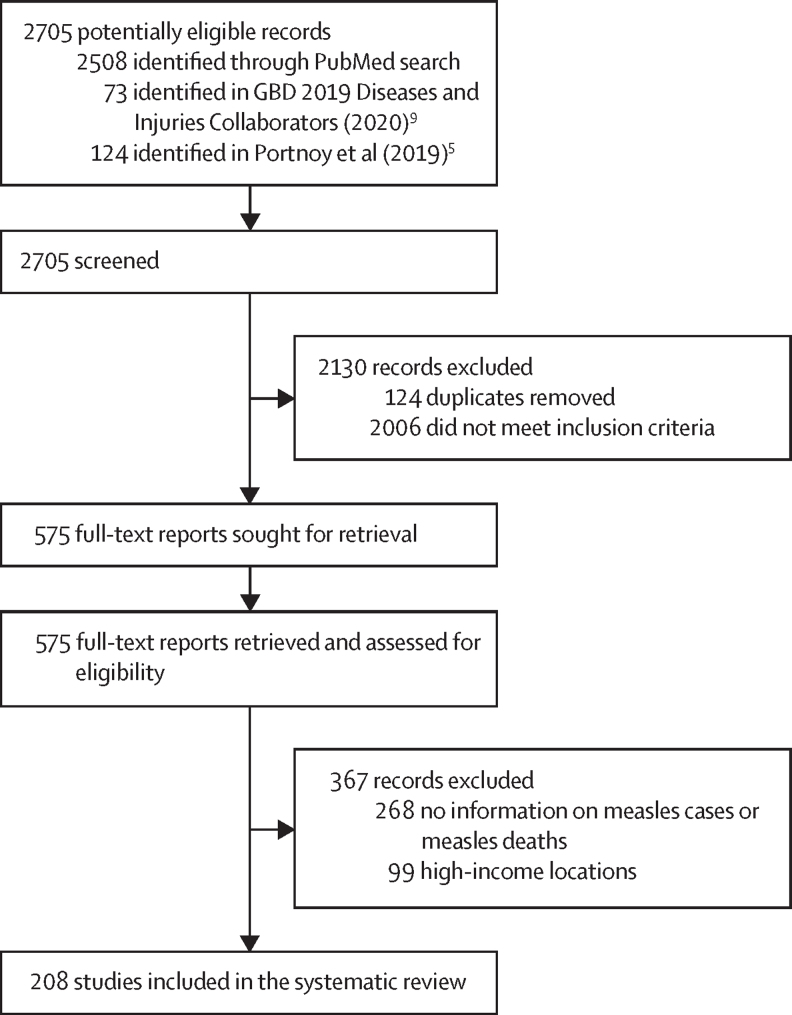
Methods: For this systematic review and meta-regression modelling study, we searched PubMed on Dec 31, 2020 for all available primary data published from Jan 1, 1980 to Dec 31, 2020, on measles cases and fatalities occurring up to Dec 31, 2019 in LMICs. We included studies that previous systematic reviews had included or which contained primary data on measles cases and deaths from hospital-based, community-based, or surveillance-based reports, including outbreak investigations. We excluded studies that were not in humans, or reported only data that were only non-primary, or on restricted populations (eg, people living with HIV), or on long-term measles mortality (eg, death from subacute sclerosing panencephalitis), and studies that did not include country-level data or relevant information on measles cases and deaths, or were for a high-income country. We extracted summary data on measles cases and measles deaths from studies that fitted our inclusion and exclusion criteria. Using these data and a suite of covariates related to measles CFRs, we implemented a Bayesian meta-regression model to produce estimates of measles CFRs from 1990 to 2019 by location and age group. This study was not registered with PROSPERO or otherwise.
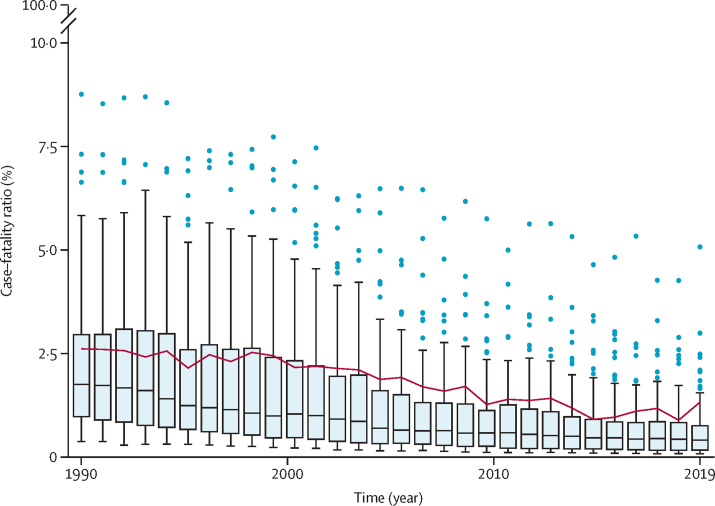
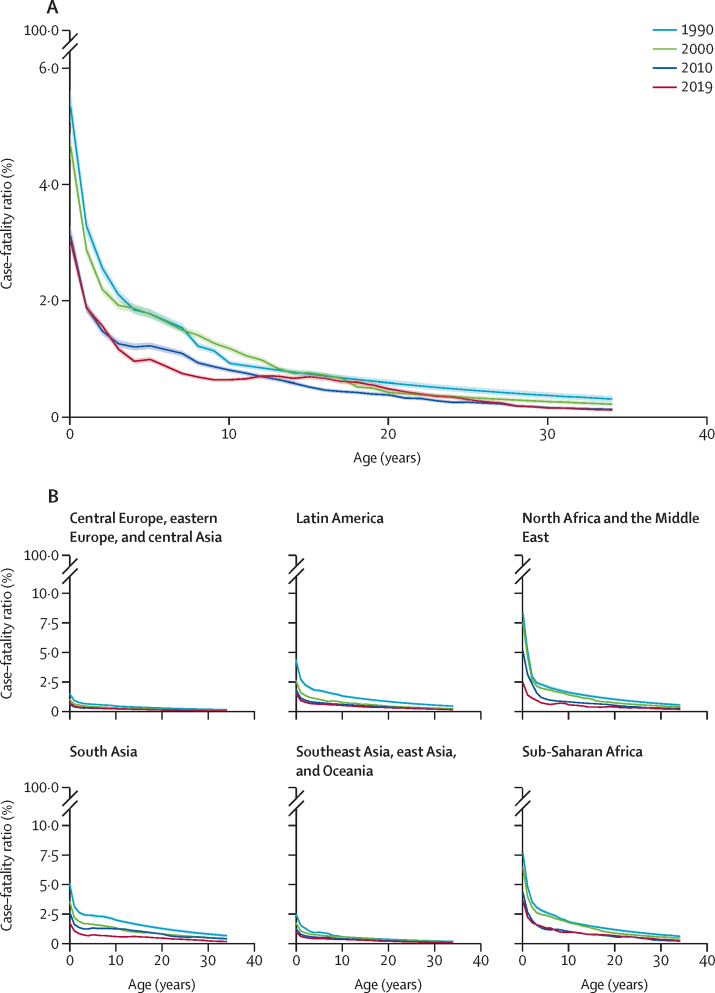
Findings: We identified 2705 records, of which 208 sources contained information on both measles cases and measles deaths in LMICS and were included in the review. Between 1990 and 2019, CFRs substantially decreased in both community-based and hospital-based settings, with consistent patterns across age groups. For people aged 0-34 years, we estimated a mean CFR for 2019 of 1·32% (95% uncertainty interval [UI] 1·28-1·36) among community-based settings and 5·35% (5·08-5·64) among hospital-based settings. We estimated the 2019 CFR in community-based settings to be 3·03% (UI 2·89-3·16) for those younger than 1 year, 1·63% (1·58-1·68) for age 1-4 years, 0·84% (0·80-0·87) for age 5-9 years, and 0·67% (0·64-0·70) for age 10-14 years.
Interpretation: Although CFRs have declined between 1990 and 2019, there are still large heterogeneities across locations and ages. One limitation of this systematic review is that we were unable to assess measles CFR among particular populations, such as refugees and internally displaced people. Our updated methodological framework and estimates could be used to evaluate the effect of measles control and vaccination programmes on reducing the preventable measles mortality burden.
Funding: Bill & Melinda Gates Foundation; Gavi, the Vaccine Alliance; and the US National Institutes of Health.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ANS, JFM, MJ, MF, RER, ELBR, and AP received funding for this work from, and LKK is employed by, the Bill & Melinda Gates Foundation. ANS received grant support from the US National Institutes of Health (NIH; F31AI167535). ANS, JFM, and MJ received grant support from Gavi. MF received grant support from WHO. PO declares no competing interests. The content of this work is the sole responsibility of the authors and does not represent the official views of the NIH.
Figures
Comment in
-
Exacerbation of measles mortality by vaccine hesitancy worldwide.Lancet Glob Health. 2023 Apr;11(4):e478-e479. doi: 10.1016/S2214-109X(23)00063-3. Lancet Glob Health. 2023. PMID: 36925157 No abstract available.
References
-
- 56th World Health Assembly Reducing global measles mortality. May 26, 2003. https://apps.who.int/iris/handle/10665/78321
-
- Wolfson LJ, Grais RF, Luquero FJ, Birmingham ME, Strebel PM. Estimates of measles case fatality ratios: a comprehensive review of community-based studies. Int J Epidemiol. 2009;38:192–205. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
