

The impact of alternative delivery strategies for novel tuberculosis vaccines in low-income and middle-income countries: a modelling study
- PMID: 36925175
- PMCID: PMC10030455
- DOI: 10.1016/S2214-109X(23)00045-1
The impact of alternative delivery strategies for novel tuberculosis vaccines in low-income and middle-income countries: a modelling study
Abstract
Background: Tuberculosis is a leading infectious cause of death worldwide. Novel vaccines will be required to reach global targets and reverse setbacks resulting from the COVID-19 pandemic. We estimated the impact of novel tuberculosis vaccines in low-income and middle-income countries (LMICs) in several delivery scenarios.
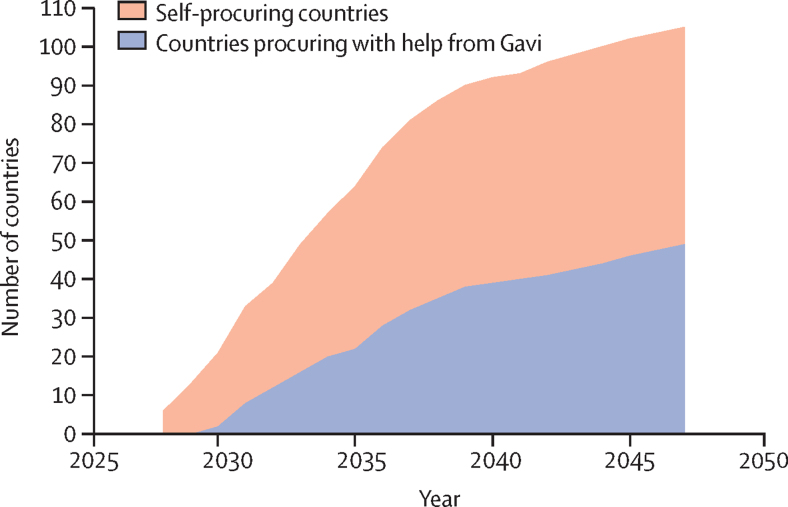
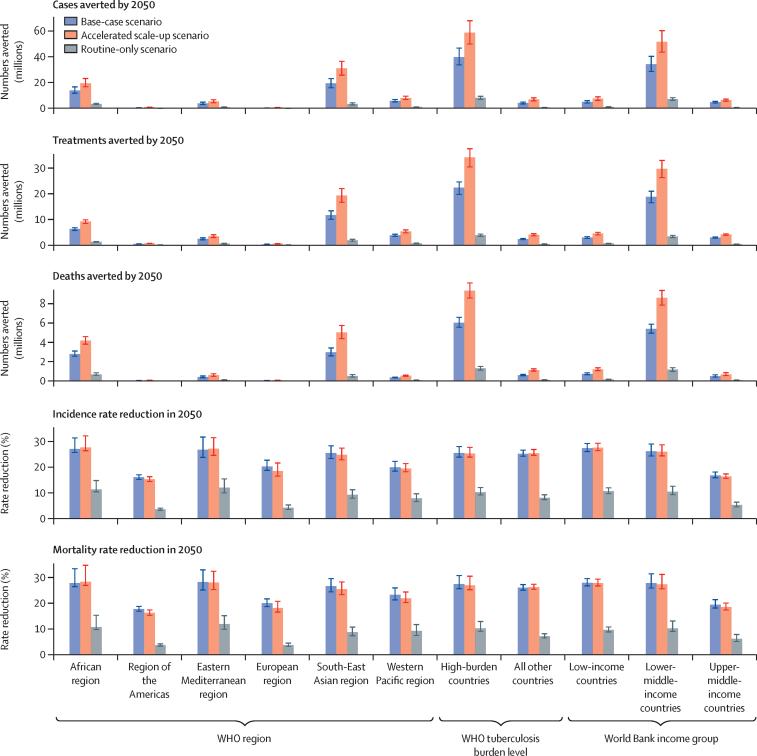
Methods: We calibrated a tuberculosis model to 105 LMICs (accounting for 93% of global incidence). Vaccine scenarios were implemented as the base-case (routine vaccination of those aged 9 years and one-off vaccination for those aged 10 years and older, with country-specific introduction between 2028 and 2047, and 5-year scale-up to target coverage); accelerated scale-up similar to the base-case, but with all countries introducing vaccines in 2025, with instant scale-up; and routine-only (similar to the base-case, but including routine vaccination only). Vaccines were assumed to protect against disease for 10 years, with 50% efficacy.
Findings: The base-case scenario would prevent 44·0 million (95% uncertainty range 37·2-51·6) tuberculosis cases and 5·0 million (4·6-5·4) tuberculosis deaths before 2050, compared with equivalent estimates of cases and deaths that would be predicted to occur before 2050 with no new vaccine introduction (the baseline scenario). The accelerated scale-up scenario would prevent 65·5 million (55·6-76·0) cases and 7·9 million (7·3-8·5) deaths before 2050, relative to baseline. The routine-only scenario would prevent 8·8 million (95% uncertainty range 7·6-10·1) cases and 1·1 million (0·9-1·2) deaths before 2050, relative to baseline.
Interpretation: Our results suggest novel tuberculosis vaccines could have substantial impact, which will vary depending on delivery strategy. Including a one-off vaccination campaign will be crucial for rapid impact. Accelerated introduction-at a pace similar to that seen for COVID-19 vaccines-would increase the number of lives saved before 2050 by around 60%. Investment is required to support vaccine development, manufacturing, prompt introduction, and scale-up.
Funding: WHO (2020/985800-0).
Translations: For the French, Spanish, Italian and Dutch translations of the abstract see Supplementary Materials section.
Copyright © 2023 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products, or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests SM reports employment by the International AIDS Vaccine Initiative, a non-profit product development partnership supporting the access-oriented development of vaccines for several disease areas, including tuberculosis, and grant funding from WHO. MJ is funded by the Bill & Melinda Gates Foundation, Gavi the Vaccine Alliance, the UK Research Institute, the National Institute for Health Research, the European Commission, and the Wellcome Trust, and reports leadership or fiduciary roles in the board, society, committee, or advocacy groups for WHO and Gavi. RCH reports employment by Sanofi Pasteur, unrelated to tuberculosis and outside the submitted work. NAM received consulting fees from The Global Fund to Fight AIDS, Tuberculosis and Malaria and WHO, and reports funding to their institution from the US Centers for Disease Control and Prevention, the Gates Foundation, the National Institute of Health, and the US Council of State and Territorial Epidemiologists. RGW is funded for other work by the Wellcome Trust (218261/Z/19/Z), the National Institute of Health (1R01AI147321–01), EDCTP (RIA208D-2505B), the UK's Medical Research Council (CCF17–7779 via SET Bloomsbury), the Economic and Social Research Council (ES/P008011/1), the Gates Foundation (OPP1084276, OPP1135288, and INV-001754), and WHO. All other authors declare no competing interests.
Figures
Comment in
-
Planning to introduce novel tuberculosis vaccines in high burden settings: how could this be done?Lancet Glob Health. 2023 Apr;11(4):e484-e485. doi: 10.1016/S2214-109X(23)00123-7. Lancet Glob Health. 2023. PMID: 36925160 Free PMC article. No abstract available.
References
-
- WHO Global tuberculosis report. 2021. https://apps.who.int/iris/handle/10665/346387
-
- WHO The End TB Strategy. Aug 16, 2015. https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19
-
- Stop TB Partnership New data shows COVID-19 combined with funding shortfalls are devastating efforts to end TB by 2030. 2021. https://www.stoptb.org/news/new-data-shows-covid-19-combined-with-fundin...
-
- WHO WHO Preferred product characteristics for new tuberculosis vaccines. 2018. https://apps.who.int/iris/bitstream/handle/10665/273089/WHO-IVB-18.06-en... - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
