

Bone Morphogenetic Protein 10-A Novel Biomarker to Predict Adverse Outcomes in Patients With Atrial Fibrillation
- PMID: 36926939
- PMCID: PMC10111531
- DOI: 10.1161/JAHA.122.028255
Bone Morphogenetic Protein 10-A Novel Biomarker to Predict Adverse Outcomes in Patients With Atrial Fibrillation
Abstract
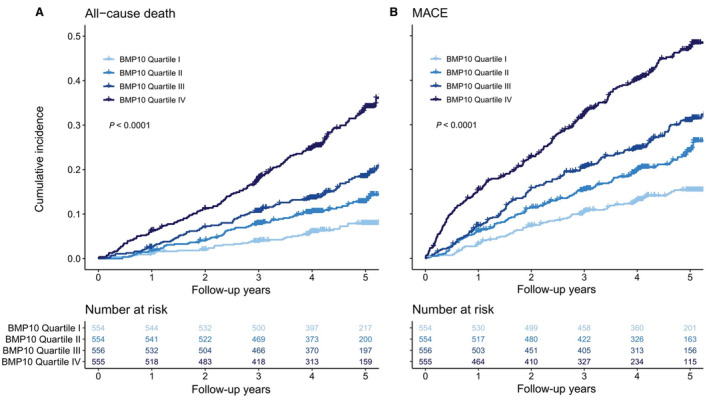
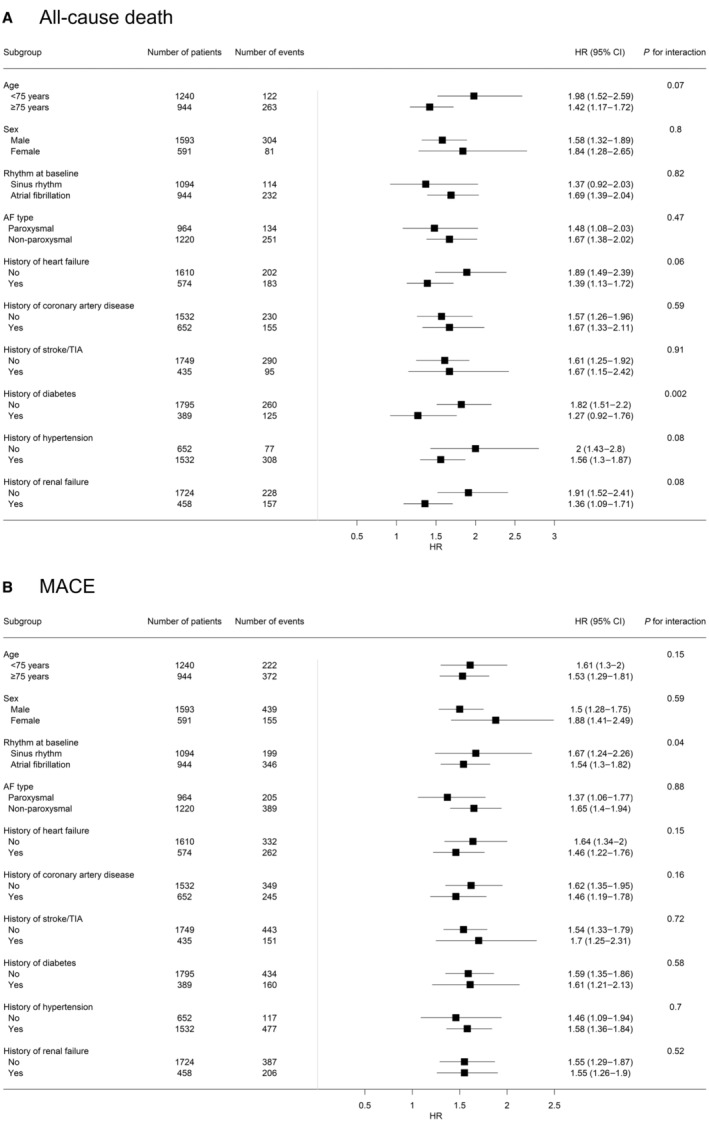
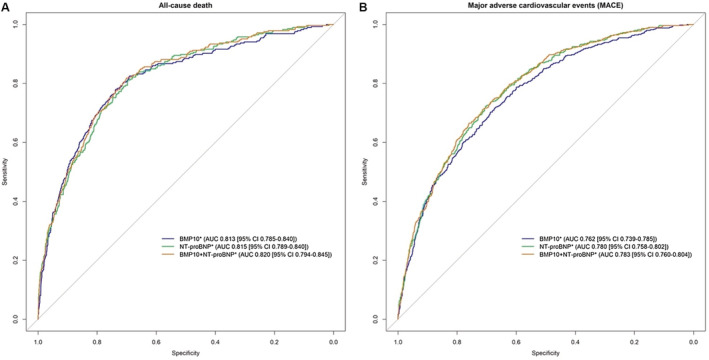
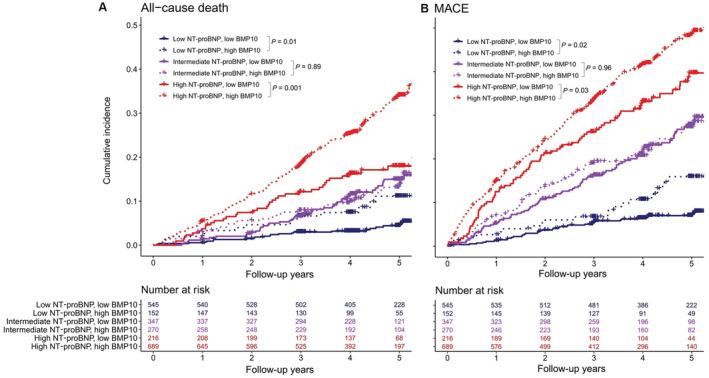
Background Patients with atrial fibrillation (AF) face an increased risk of death and major adverse cardiovascular events (MACE). We aimed to assess the predictive value of the novel atrial-specific biomarker BMP10 (bone morphogenetic protein 10) for death and MACE in patients with AF in comparison with NT-proBNP (N-terminal prohormone of B-type natriuretic peptide). Methods and Results BMP10 and NT-proBNP were measured in patients with AF enrolled in Swiss-AF (Swiss Atrial Fibrillation Study), a prospective multicenter cohort study. A total of 2219 patients were included (median follow-up 4.3 years [interquartile range 3.9, 5.1], mean age 73±9 years, 73% male). In multivariable Cox proportional hazard models, the adjusted hazard ratio (aHR) associated with 1 ng/mL increase of BMP10 was 1.60 (95% CI, 1.37-1.87) for all-cause death, and 1.54 (95% CI, 1.35-1.76) for MACE. For all-cause death, the concordance index was 0.783 (95% CI, 0.763-0.809) for BMP10, 0.784 (95% CI, 0.765-0.810) for NT-proBNP, and 0.789 (95% CI, 0.771-0.815) for both biomarkers combined. For MACE, the concordance index was 0.732 (95% CI, 0.715-0.754) for BMP10, 0.747 (95% CI, 0.731-0.768) for NT-proBNP, and 0.750 (95% CI, 0.734-0.771) for both biomarkers combined. When grouping patients according to NT-proBNP categories (<300, 300-900, >900 ng/L), higher aHRs were observed in patients with high BMP10 in the categories of low NT-proBNP (all-cause death aHR, 2.28 [95% CI, 1.15-4.52], MACE aHR, 1.88 [95% CI, 1.07-3.28]) and high NT-proBNP (all-cause death aHR, 1.61 [95% CI, 1.14-2.26], MACE aHR, 1.38 [95% CI, 1.07-1.80]). Conclusions BMP10 strongly predicted all-cause death and MACE in patients with AF. BMP10 provided additional prognostic information in low- and high-risk patients according to NT-proBNP stratification. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02105844.
Keywords: BMP10; MACE; atrial fibrillation; bone morphogenetic protein 10; death.
Figures
References
-
- Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Njølstad I, Vartiainen E, Sans S, Pasterkamp G, Hughes M, et al. Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the BiomarCaRE consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation. 2017;136:1588–1597. doi: 10.1161/CIRCULATIONAHA.117.028981 - DOI - PMC - PubMed
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström‐Lundqvist C, Boriani G, Castella M, Dan G‐A, Dilaveris PE, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio‐Thoracic Surgery (EACTS). Eur Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
