

Exploring preconception signatures of metabolites in mothers with gestational diabetes mellitus using a non-targeted approach
- PMID: 36927416
- PMCID: PMC10022116
- DOI: 10.1186/s12916-023-02819-5
Exploring preconception signatures of metabolites in mothers with gestational diabetes mellitus using a non-targeted approach
Abstract
Background: Metabolomic changes during pregnancy have been suggested to underlie the etiology of gestational diabetes mellitus (GDM). However, research on metabolites during preconception is lacking. Therefore, this study aimed to investigate distinctive metabolites during the preconception phase between GDM and non-GDM controls in a nested case-control study in Singapore.
Methods: Within a Singapore preconception cohort, we included 33 Chinese pregnant women diagnosed with GDM according to the IADPSG criteria between 24 and 28 weeks of gestation. We then matched them with 33 non-GDM Chinese women by age and pre-pregnancy body mass index (ppBMI) within the same cohort. We performed a non-targeted metabolomics approach using fasting serum samples collected within 12 months prior to conception. We used generalized linear mixed model to identify metabolites associated with GDM at preconception after adjusting for maternal age and ppBMI. After annotation and multiple testing, we explored the additional predictive value of novel signatures of preconception metabolites in terms of GDM diagnosis.
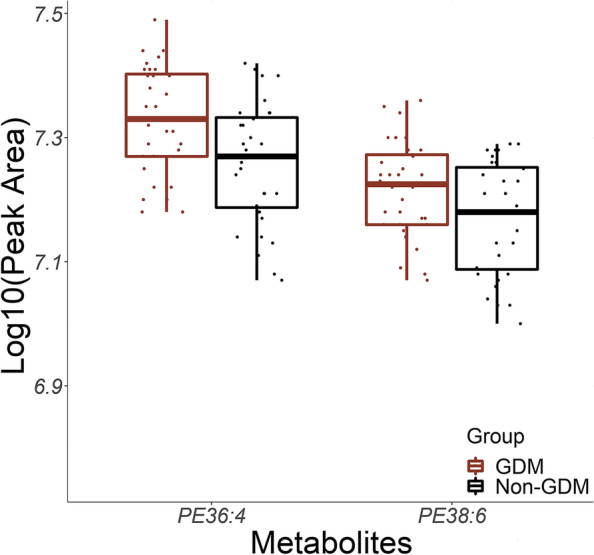
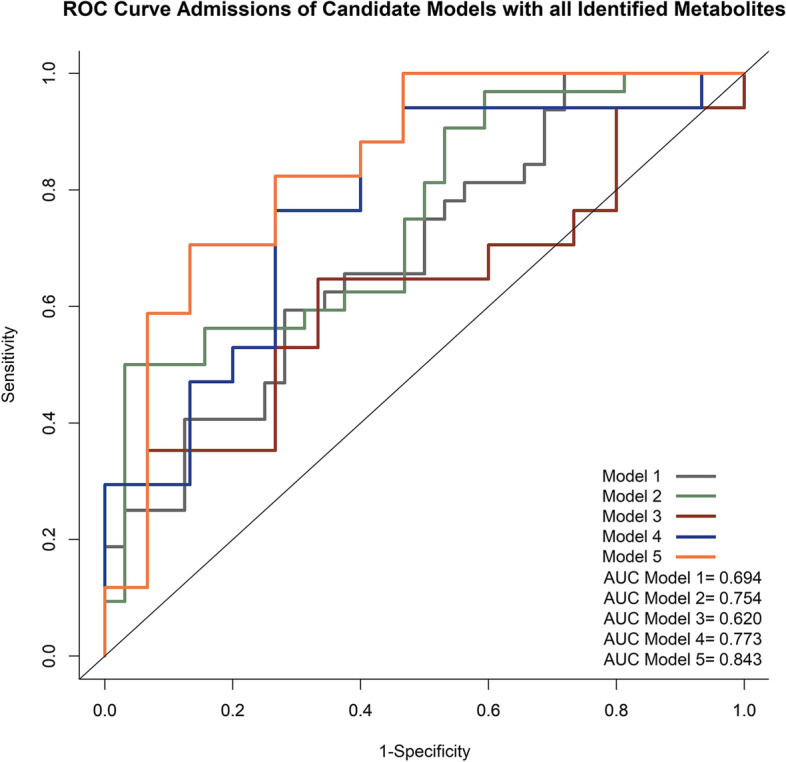
Results: A total of 57 metabolites were significantly associated with GDM, and eight phosphatidylethanolamines were annotated using HMDB. After multiple testing corrections and sensitivity analysis, phosphatidylethanolamines 36:4 (mean difference β: 0.07; 95% CI: 0.02, 0.11) and 38:6 (β: 0.06; 0.004, 0.11) remained significantly higher in GDM subjects, compared with non-GDM controls. With all preconception signals of phosphatidylethanolamines in addition to traditional risk factors (e.g., maternal age and ppBMI), the predictive value measured by area under the curve (AUC) increased from 0.620 to 0.843.
Conclusions: Our data identified distinctive signatures of GDM-associated preconception phosphatidylethanolamines, which is of potential value to understand the etiology of GDM as early as in the preconception phase. Future studies with larger sample sizes among alternative populations are warranted to validate the associations of these signatures of metabolites and their predictive value in GDM.
Keywords: Gestational diabetes mellitus; Lipids; Metabolites; Non-targeted metabolomics; Phosphatidylethanolamines; Preconception; Prediction.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
