

First-in-human phase I study of the OX40 agonist GSK3174998 with or without pembrolizumab in patients with selected advanced solid tumors (ENGAGE-1)
- PMID: 36927527
- PMCID: PMC10030671
- DOI: 10.1136/jitc-2022-005301
First-in-human phase I study of the OX40 agonist GSK3174998 with or without pembrolizumab in patients with selected advanced solid tumors (ENGAGE-1)
Abstract
Background: The phase I first-in-human study ENGAGE-1 evaluated the humanized IgG1 OX40 agonistic monoclonal antibody GSK3174998 alone (Part 1 (P1)) or in combination with pembrolizumab (Part 2 (P2)) in patients with advanced solid tumors.
Methods: GSK3174998 (0.003-10 mg/kg) ± pembrolizumab (200 mg) was administered intravenously every 3 weeks using a continuous reassessment method for dose escalation. Primary objectives were safety and tolerability; secondary objectives included pharmacokinetics, immunogenicity, pharmacodynamics, and clinical activity.
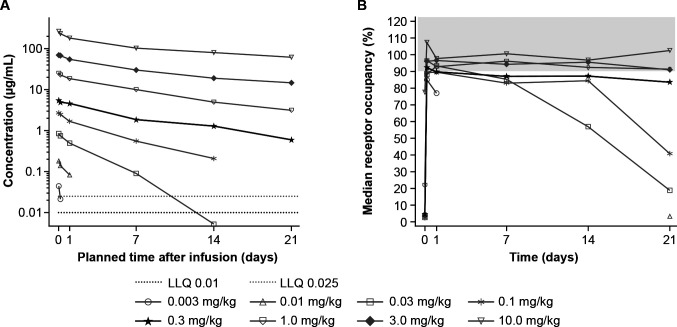
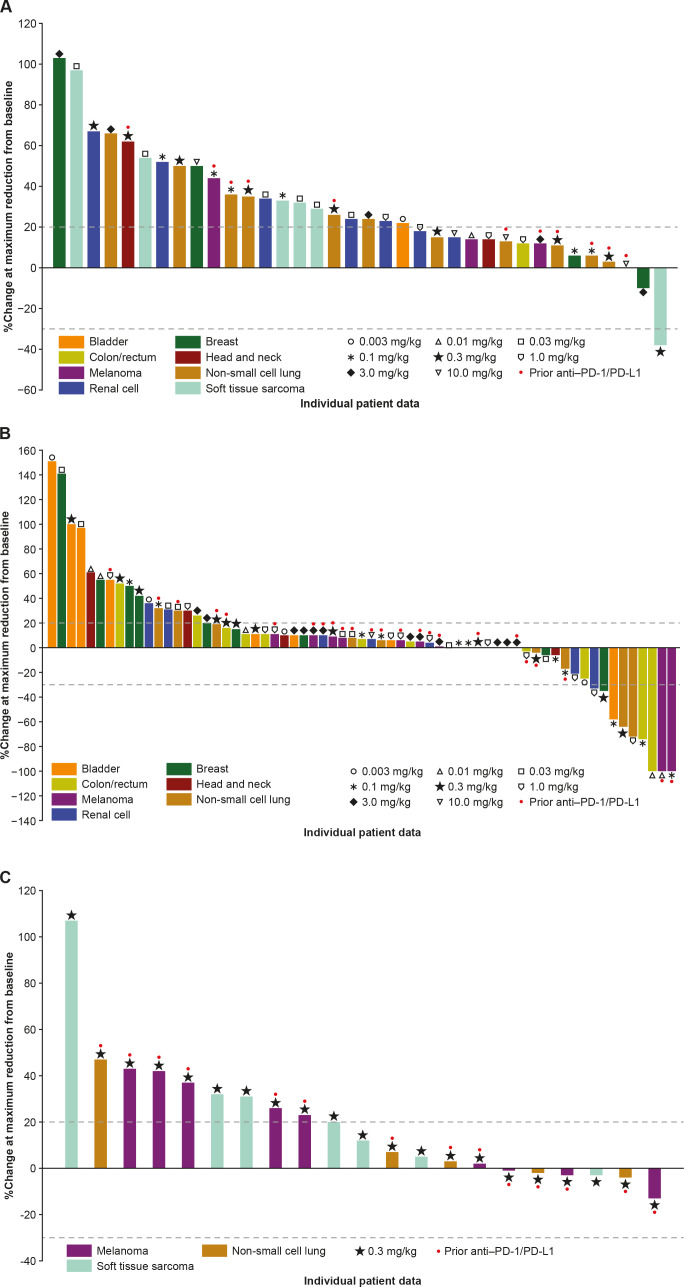
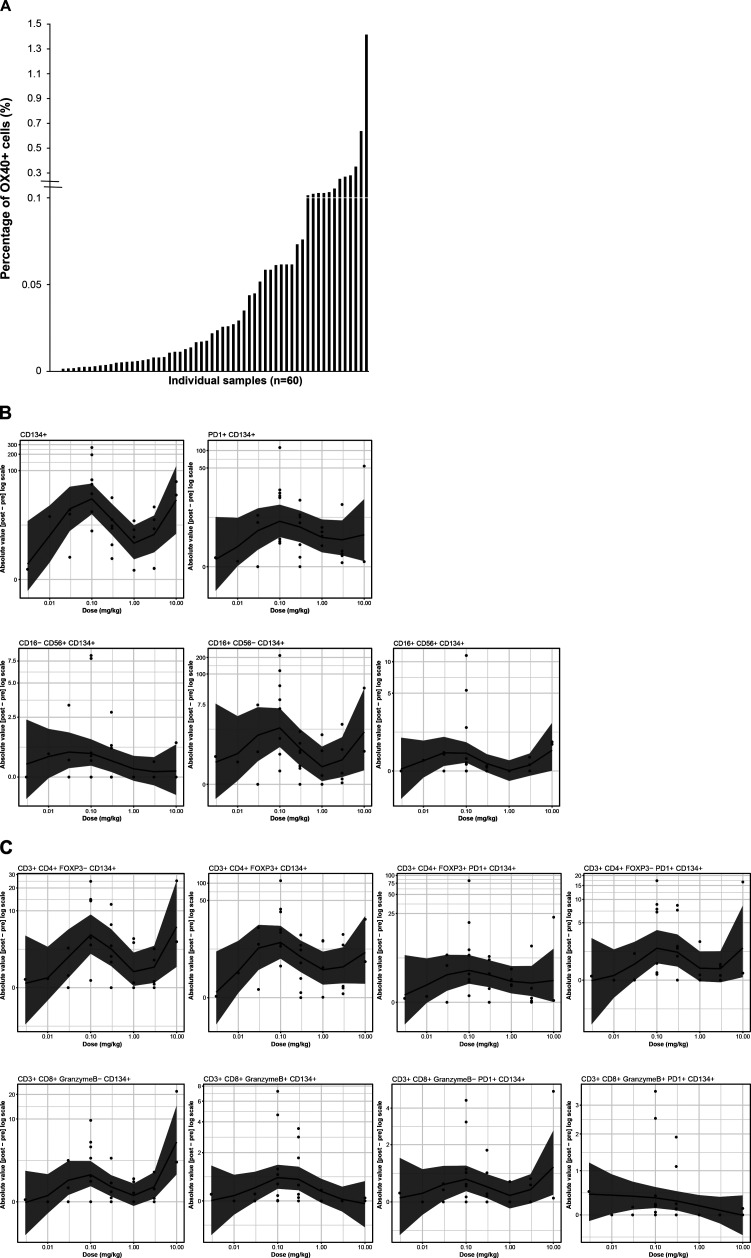
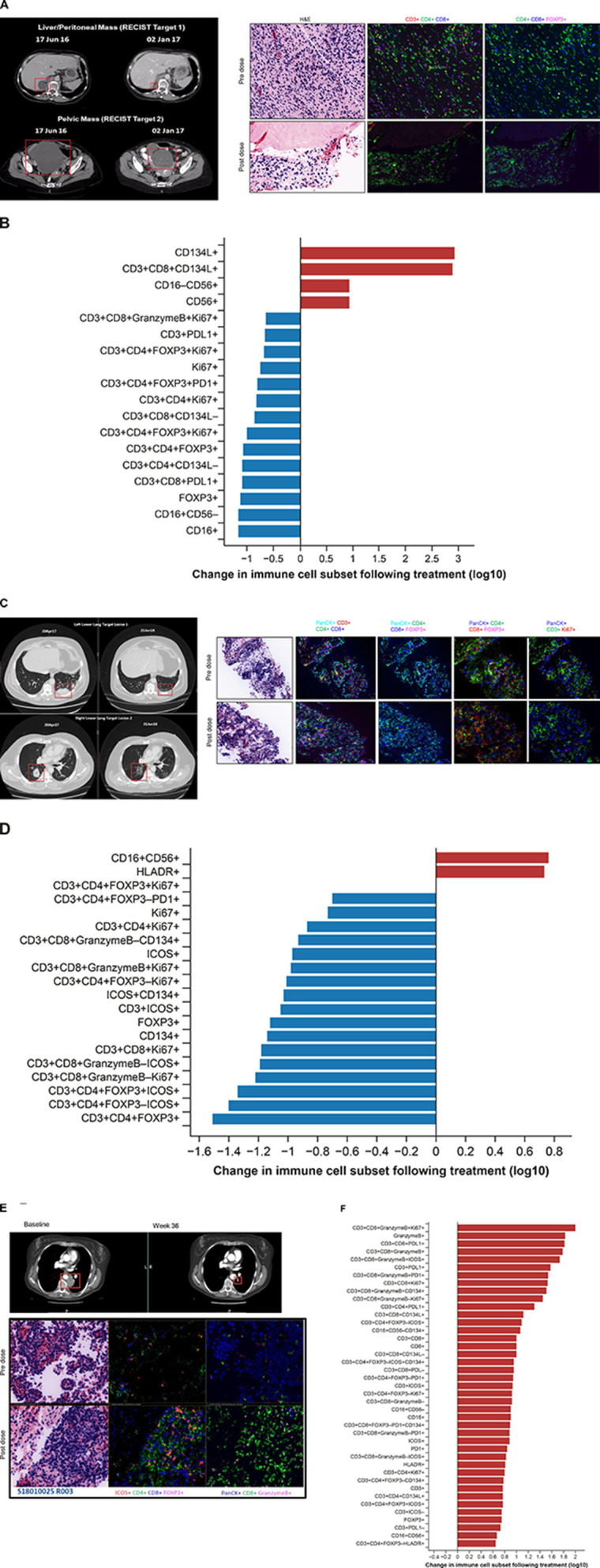
Results: 138 patients were enrolled (45 (P1) and 96 (P2, including 3 crossovers)). Treatment-related adverse events occurred in 51% (P1) and 64% (P2) of patients, fatigue being the most common (11% and 24%, respectively). No dose-toxicity relationship was observed, and maximum-tolerated dose was not reached. Dose-limiting toxicities (P2) included Grade 3 (G3) pleural effusion and G1 myocarditis with G3 increased troponin. GSK3174998 ≥0.3 mg/kg demonstrated pharmacokinetic linearity and >80% receptor occupancy on circulating T cells; 0.3 mg/kg was selected for further evaluation. Limited clinical activity was observed for GSK3174998 (P1: disease control rate (DCR) ≥24 weeks 9%) and was not greater than that expected for pembrolizumab alone (P2: overall response rate 8%, DCR ≥24 weeks 28%). Multiplexed immunofluorescence data from paired biopsies suggested that increased infiltration of natural killer (NK)/natural killer T (NKT) cells and decreased regulatory T cells (Tregs) in the tumor microenvironment may contribute to clinical responses: CD16+CD56-CD134+ NK /NKT cells and CD3+CD4+FOXP3+CD134+ Tregs exhibited the largest magnitude of change on treatment, whereas CD3+CD8+granzyme B+PD-1+CD134+ cytotoxic T cells were the least variable. Tumor gene expression profiling revealed an upregulation of inflammatory responses, T-cell proliferation, and NK cell function on treatment with some inflammatory cytokines upregulated in peripheral blood. However, target engagement, evidenced by pharmacologic activity in peripheral blood and tumor tissue, did not correlate with clinical efficacy. The low number of responses precluded identifying a robust biomarker signature predictive of response.
Conclusions: GSK3174998±pembrolizumab was well tolerated over the dose range tested and demonstrated target engagement. Limited clinical activity does not support further development of GSK3174998±pembrolizumab in advanced cancers.
Trial registration number: NCT02528357.
Keywords: antibodies, neoplasm; biomarkers, tumor; clinical trials as topic; costimulatory and inhibitory T-cell receptors; immunotherapy.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SP-V is a principal/subinvestigator of clinical trials for AbbVie, Adaptimmune, Adlai Nortye USA Inc, Aduro Biotech, Agios Pharmaceuticals, Amgen, Argenx BVBA, Arno Therapeutics, Astex Pharmaceuticals, AstraZeneca A, Aveo, Basilea Pharmaceutica International Ltd, Bayer Healthcare AG, BBB Technologies BV, Beigene, BicycleTx Ltd, Bioalliance Pharma, Blueprint Medicines, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol Myers Squibb, Celgene Corporation, Chugai Pharmaceutical Co, Cullinan-Apollo, Curevarc, Daiichi Sankyo, Debiopharm, Eisai, Eisai Limited, Eli Lilly, Exelixis, Faron Pharmaceuticals Ltd, Forma Tharapeutics, GamaMabs, Genentech, GSK, H3 Biomedicine, Hoffmann La Roche AG, Imcheck Therapeutics, Innate Pharma, Institut De Recherche Pierre Fabre, Iris Servier, Iteos Belgium SA, Janssen Cilag, Janssen Research Foundation, Kura Oncology, Kyowa Kirin Pharm. Dev, Lilly France, Loxo Oncology, Lytix Biopharma AS, Medimmune, Menarini Ricerche, Merck Sharp & Dohme Chibret, Merus, Molecular Partners AG, Nanobiotix, Nektar Therapeutics, Novartis Pharma, Octimet Oncology NV, Oncoethix, Oncopeptides, Onyx Therapeutics, Orion Pharma, Oryzon Genomics, Ose Pharma, Pfizer, Pharma Mar, Pierre Fabre Medicament, Plexxikon, Roche, Sanofi Aventis, Seattle Genetics, Sotio A.S, Syros Pharmaceuticals, Taiho Pharma, Tesaro, Turning Point Therapeutics, and Xencor outside the submitted work; non-financial support (drug supplied) from AstraZeneca, Bayer, Bristol Myers Squibb, Boehringer Ingelheim, GSK, Medimmune, Merck, NH TherAGuiX, Pfizer, Roche; research funding from Boehringer Ingelheim, AstraZeneca, Roche, and Merck KGaA for projects unrelated to this manuscript. VL reports consulting for Takeda, Seattle Genetics, Bristol Myers Squibb, AstraZeneca, Guardant Health; research funding from GSK, Bristol Myers Squibb, Merck, Seattle Genetics. WR reports nothing to disclose. TMB reports consulting for Guardant Health, Loxo Pharmaceuticals, Pfizer, Exelixis, Blueprint Medicines, Foundation Medicine, Bayer, AstraZeneca, Ignyta, Moderna Therapeutics, Pfizer. Speakers Bureau: Bayer, Bristol Myers Squibb, and Lilly; research funding from Daiichi Sankyo, Medpacto, Inc., Incyte, Mirati Therapeutics, MedImmune, AbbVie, AstraZeneca, Leap Therapeutics, MabVax, Stemline Therapeutics, Merck, Lilly, GSK, Novartis, Pfizer, Genentech/Roche, Deciphera, Merrimack, Immunogen, Millennium Pharmaceuticals, Ignyta, Calithera Biosciences, Kolltan Pharmaceuticals, Principa Biopharma, Peleton, Immunocore, Aileron Therapeutics, Bristol Myers Squibb, Amgen, Moderna Therapeutics, Sanofi, Boehringer Ingelheim, Astellas Pharma, Five Prime Therapeutics, Jacobio, Top Alliance BioScience, Loxo, Janssen, Clovis Oncology, Takeda, Karyopharm Therapeutics, Onyx, Phosplatin Therapeutics, Foundation Medicine, and ARMO BioScience; personal expenses from Astellas Pharma, AstraZeneca, Celgene, Clovis Oncology, EMD Serono, Genentech, Lilly, Merck, Novartis, Pharmacyclics, Sysmex, and Pfizer. AHa reports research funding from Genentech/Roche, Merck, GSK, Bristol Myers Squibb, Novartis, Boston Biomedical, Boehringer Ingelheim, AstraZeneca/Medimmune Eisai; personal fees from Merck and GSK. DCC is a consultant for Nektar, Pfizer, Werewolf, and HUYA. FSH reports research funding from Bristol Myers Squibb and Novartis; receives personal fees from Bristol Myers Squibb, Merck, EMD Serono, Novartis, Surface, Compass Therapeutics, Apricity, Sanofi, Pionyr, Torque, Bicara, Checkpoint Therapeutics, Genentech/Roche, Bioentre, Gossamer, Iovance, Trillium, Catalym, Immunocore, Amgen, Kairos, Eisai, and Rheos. JHMS is a shareholder and part-time employee of Modra Pharmaceuticals BV and patent holder of oral taxanes; reports consulting for Debiopharm. JKL reports other from GSK, Novartis, Medivation/Pfizer, Genentech, EMD-Serono, AstraZeneca, Medimmune, Zenith, Ayala, UpToDate review panels for NCCN, ASCO, NIH PDQ, Medlearning, Physicians Education Resource, Prime Oncology, Medscape, Clinical Care Options, Medpage. SA reports advisory board participation for MSD, Sanofi, Roche, Bristol Myers Squibb, Pfizer; research support from Sanofi. KAA reports research funding (to institution) from Pfizer, AstraZeneca, Amgen, Trishula, GSK, Merck, and Eli Lilly. FO is a principal/subinvestigator of clinical trials for Amgen, AstraZeneca, Cytovation, GSK, Lilly, MSD, Revmed, Incyte, Boehringer Ingelheim, Bristol Myers Squibb, Roche/Genentech, Exelexis, Relay, and InterRNA. MM reports research funding from Alpine Immune Sciences, Arcus Biosciences, Arvinas, Ascentage Pharma Group, Bayer, Bicycle Therapeutics, BioMed Valley Discoveries, BioNTech, Dragonfly Therapeutics, EMD Serono, Epizyme, Erasca, Exelixis, Foghorn Therapeutics, Genentech, Gilead Sciences, GSK, IDEAYA Biosciences, Ikena Oncology, ImmVira Pharma, Infinity Pharmaceuticals, Jacobio Pharmaceuticals, Kechow Pharma, Kezar Life Sciences, Kinnate BioPharma, MedImmune, Mereo BioPharma, Metabomed, Moderna, NBE Therapeutics, Nektar, Novartis, Oncorus, PACT Pharma, Pfizer, Plexxikon, Prelude Therapeutics, Pyramid Biosciences, Regeneron, Sapience Therapeutics, Scholar Rock Seattle Genetics, Synthrox, Takeda Pharmaceuticals, Teneobio, Tempest Therapeutics, Tizona Therapeutics, TMUNITY Therapeutics, TopAlliance Biosciences, and Xilio. M; consulting/advisory role for Astellas Pharma, AstraZeneca, BicycleTX Limited, Castle Biosciences, Eisai, Ideaya Biosciences, iTeos, Pfizer, and Regeneron Pharmaceuticals. NS reports consulting/advisory role for Deciphera, AADi, Blueprint Medicines, Bayer, Epizyme, and Boehringer Ingelheim; research funding from GSK, Karyopharm, Deciphera, Ascentage Pharma, Daiichi Sankyo/Lilly, and AstraZeneca/MedImmune. SC is the principal/subinvestigator of clinical trials for AbbVie, Adaptimmune, Adlai Nortye USA Inc, Aduro Biotech, Agios Pharmaceuticals, Amgen, Astex Pharmaceuticals, AstraZeneca AB, Aveo, Basilea Pharmaceutica International Ltd, Bayer Healthcare AG, BBB Technologies BV, Beigene, BicycleTx Ltd, Blueprint Medicines, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol Myers Squibb, Casi Pharmaceuticals, Inc, Celgene Corporation (a Bristol-Myers Squibb company), Cellcentric, Chugai Pharmaceutical Co, Cullinan-Apollo, Curevarc, Cytovasion, Daiichi Sankyo, Debiopharm, Eisai, Eli Lilly, Exelixis, Faron Pharmaceuticals Ltd, Forma Tharapeutics, GamaMabs, Genentech, GSK, H3 Biomedicine, Hoffmann La Roche AG, Imcheck Therapeutics, Incyte Corporation, Innate Pharma, Institut De Recherche Pierre Fabre, Iris Servier, Iteos Belgium SA, Janssen Cilag, Janssen Research Foundation, Janssen R&D LLC, Kura Oncology, Kyowa Kirin Pharm. Dev, Lilly France, Loxo Oncology, Medimmune, Menarini Ricerche, Merck, Merck Sharp & Dohme Chibret, Merrimack Pharmaceuticals, Merus, Molecular Partners AG, Nanobiotix, Nektar Therapeutics, Novartis Pharma, Octimet Oncology NV, Oncoethix, Oncopeptides, Orion Pharma, Genomics, Ose Pharma, Pfizer, Pharma Mar, Pierre Fabre Medicament, Relay Therapeutics, Inc, Roche, Sanofi Aventis, Seattle Genetics, Sotio, Syros Pharmaceuticals, Taiho Pharma, Tesaro, Transgene SA, Turning Point Therapeutics, and Xencor; reports research grants from AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, GSK, INCA, Janssen Cilag, Merck, Pfizer, Roche, and Sanofi; reports non-financial support (drug supplied) from AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, GSK, Medimmune, Merck, NH TherAGuiX, Pfizer, and Roche; reports honoraria from Amgen, Astellas, AstraZeneca, Bristol Myers Squibb, Eisai, Genmab, Janssen, Merck, Novartis and Roche; reports participation in advisory boards for Alderaan Biotechnology, Amgen, AstraZeneca, Avacta, Ellipses Pharma, Oncovita, Seagen, UltraHuman8; reports travel and congress support from AstraZeneca, Bristol Myers Squibb, Merck, Ose Pharma, Roche, Sotio. MA reports research funding (to institution) from Genentech, Nektar Therapeutics, Merck, GSK, Novartis, Jounce Therapeutics, Bristol Myers Squibb, Eli Lilly, Adaptimmune, Shattuck Lab, and Gilead. Advisory boards: GSK, Shattuck Lab, Bristol Myers Squibb, AstraZeneca; reports speaker fees from AstraZeneca, and Nektar Therapeutics. AS reports participation in advisory boards for Merck, Bristol Myers Squibb, Novartis, Oncorus, Janssen, Medison, and Immunocore; reports research support: Novartis, Bristol Myers Squibb, Symphogen AstraZeneca/Medimmune, Merck, Bayer, Surface Oncology, Northern Biologics, Janssen Oncology/Johnson & Johnson, Roche, Regeneron, Alkermes, Array Biopharma/Pfizer, GSK, Treadwell, and Amgen. OR reports employment with AstraZeneca; reports research funding from Merck; reports speaker for activities supported by educational grants from Bristol Myers Squibb and Merck; reports consulting for Merck, Celgene, Five Prime, GSK, Bayer, Roche/Genentech, Puretech, Imvax, Sobi, Boehringer Ingelheim; reports pending patent for “Methods of using pembrolizumab and trebananib”. EMP, CMA, HZ, HS, SAG, MW, KMY, NY, and AHo report employment with GSK. MJC is an employee of Merck and owns stock. EVS is an employee of Merck. AM has been a principal or coinvestigator of clinical trials using OX40-targeted agents and/or has provided consulting services for Roche/Genentech, AstraZeneca, Pfizer, GSK, HiFiBiO, Bristol Myers Squibb, Shattuck Labs. JW reports consulting for Merck, Genentech, AstraZeneca, GSK, Novartis, Nektar, Celldex, Incyte, Biond, ImCheck, Sellas, Evaxion and EMD Serono; reports participation in advisory boards for Bristol Myers Squibb (compensated), CytoMx, Incyte, ImCheck, Biond, Sellas, Instil Bio, OncoC4, and Neximmune; reports equity holdings in Biond, Evaxion, Instil Bio, OncoC4, and Neximmune; reports research support (to institution) from Bristol Myers Squibb, Merck, GSK, Moderna, Pfizer, Novartis, and AstraZeneca, Moffitt Cancer Center; reports patent for ipilimumab biomarker and tumor-infiltrating lymphocytes preparation and a PD-1 patent (Biodesix). JVH reports other from GSK, AstraZeneca, Checkmate Pharmaceuticals, Brightpath Biotherapeutics, Eli Lilly & Co, Kairos Venture Investments, Triptych Health Partners; reports patent with Spectrum Pharmaceuticals.
Figures
References
-
- Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc . Keytruda (pembrolizumab) [package insert]. Rahway, NJ, USA, 2021.
-
- Bristol Myers Squibb Company . Yervoy (ipilimumab) [package insert]. Princeton, NJ, 2021.
-
- Bristol Myers Squibb Company . Opdivo (nivolumab) [package insert]. Princeton, NJ, 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials