

Immune landscape in invasive ductal and lobular breast cancer reveals a divergent macrophage-driven microenvironment
- PMID: 36927792
- PMCID: PMC11194444
- DOI: 10.1038/s43018-023-00527-w
Immune landscape in invasive ductal and lobular breast cancer reveals a divergent macrophage-driven microenvironment
Erratum in
-
Publisher Correction: Immune landscape in invasive ductal and lobular breast cancer reveals a divergent macrophage-driven microenvironment.Nat Cancer. 2023 Apr;4(4):582. doi: 10.1038/s43018-023-00549-4. Nat Cancer. 2023. PMID: 37012402 No abstract available.
Abstract
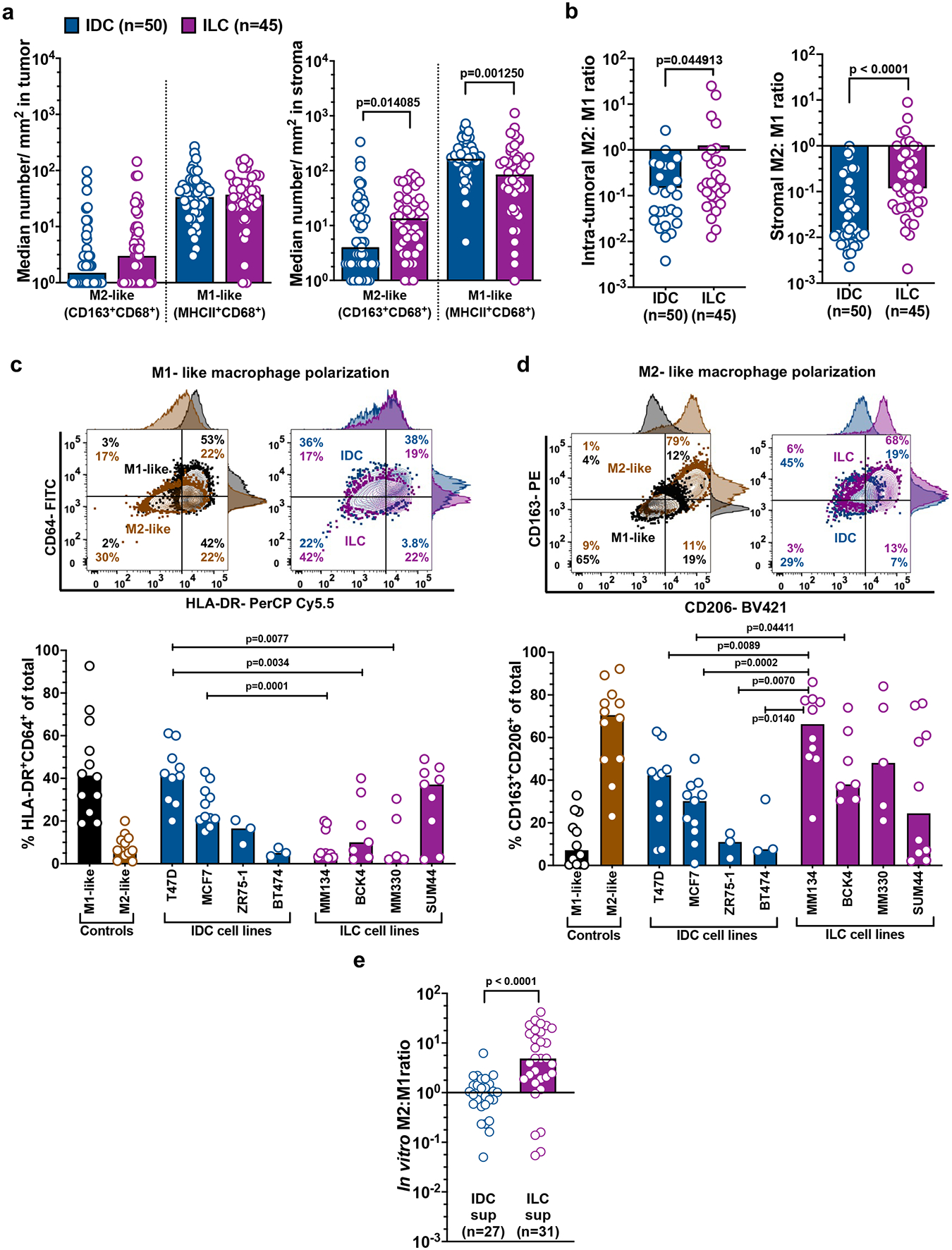
T cell-centric immunotherapies have shown modest clinical benefit thus far for estrogen receptor-positive (ER+) breast cancer. Despite accounting for 70% of all breast cancers, relatively little is known about the immunobiology of ER+ breast cancer in women with invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC). To investigate this, we performed phenotypic, transcriptional and functional analyses for a cohort of treatment-naive IDC (n = 94) and ILC (n = 87) tumors. We show that macrophages, and not T cells, are the predominant immune cells infiltrating the tumor bed and the most transcriptionally diverse cell subset between IDC and ILC. Analysis of cellular neighborhoods revealed an interplay between macrophages and T cells associated with longer disease-free survival in IDC but not ILC. Our datasets provide a rich resource for further interrogation into immune cell dynamics in ER+ IDC and ILC and highlight macrophages as a potential target for ER+ breast cancer.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
D.A.A.V. is cofounder and stockholder of Novasenta, Potenza, Tizona and Trishula; stock holder of Oncorus, Werewolf and Apeximmune; has patents licensed and royalties from Astellas, BMS, Novasenta; scientific advisory board member of Tizona, Werewolf, F-Star, Bicara, Apeximmune and T7/Imreg Bio; is a consultant for Astellas, BMS, Almirall, Incyte, G1 Therapeutics and Inzen Therapeutics; and obtained research funding from BMS, Astellas and Novasenta. All authors declare no competing financial or non-financial interests in relation to the work submitted in this manuscript.
Figures
















References
-
- Pestalozzi BC, Z. D, Mallon E, Gusterson BA, Price KN, Gelber RD et al. , Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 International Breast Cancer Study Group clinical trials. J Clin Oncol, 2008. 20; 26(18):3006–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
