

Model-based economic evaluation of the effectiveness of "'Hypos' can strike twice", a leaflet-based ambulance clinician referral intervention to prevent recurrent hypoglycaemia
- PMID: 36928118
- PMCID: PMC10019663
- DOI: 10.1371/journal.pone.0282987
Model-based economic evaluation of the effectiveness of "'Hypos' can strike twice", a leaflet-based ambulance clinician referral intervention to prevent recurrent hypoglycaemia
Abstract
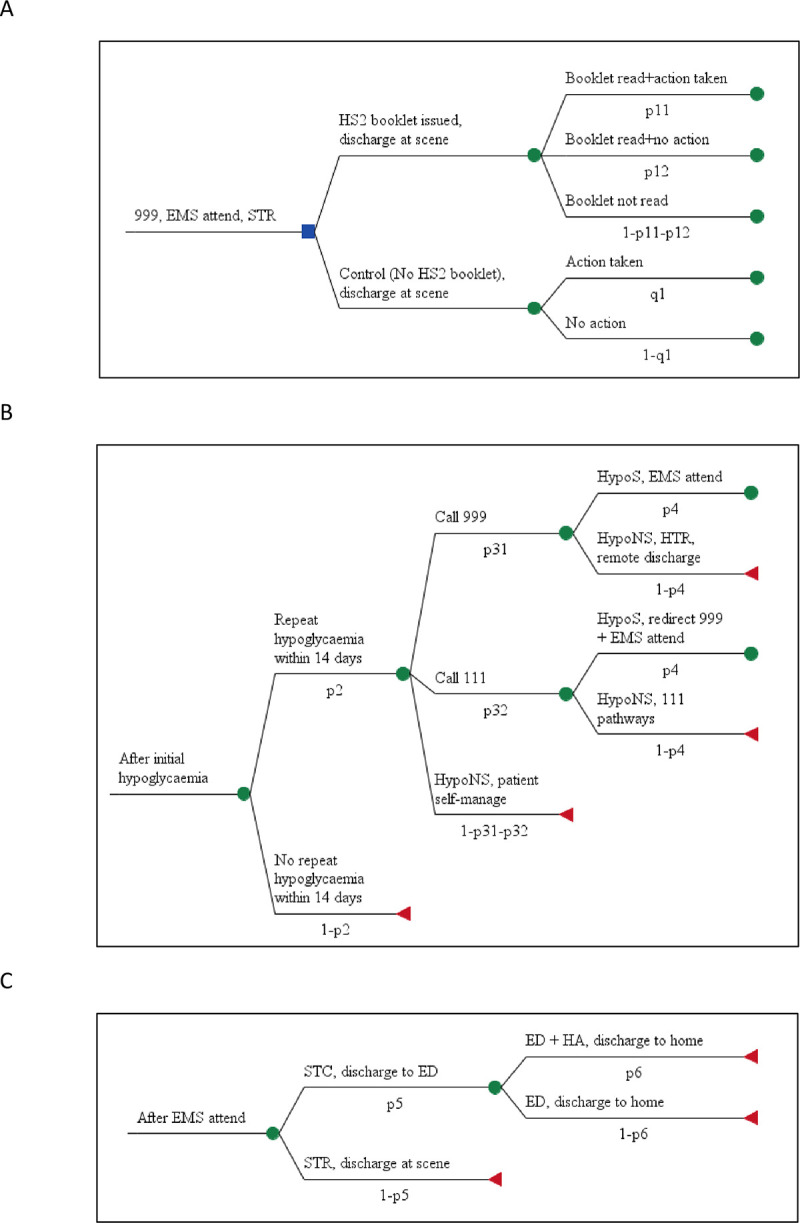
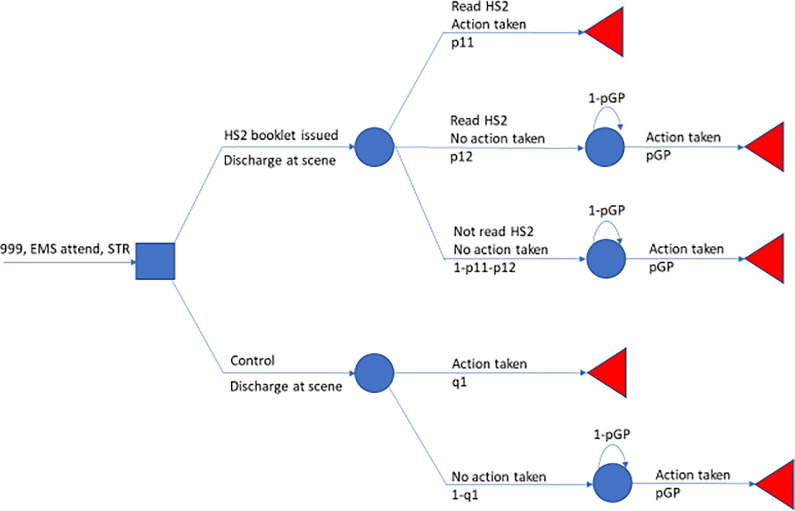
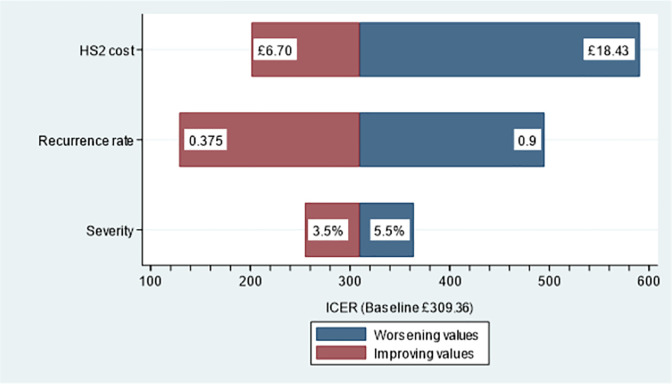
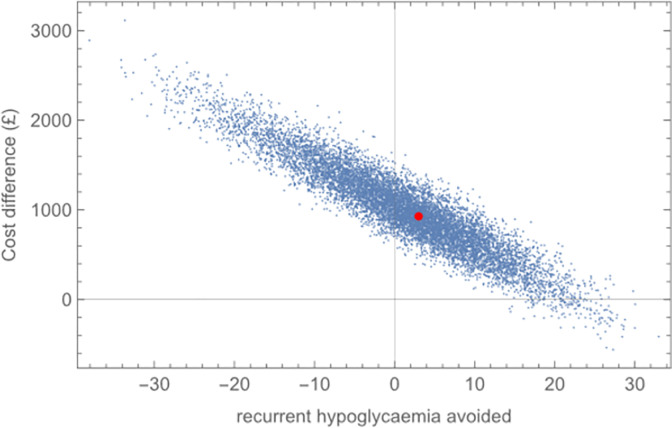
"'Hypos' can strike twice" (HS2) is a pragmatic, leaflet-based referral intervention designed for administration by clinicians of the emergency medical services (EMS) to people they have attended and successfully treated for hypoglycaemia. Its main purpose is to encourage the recipient to engage with their general practitioner or diabetic nurse in order that improvements in medical management of their diabetes may be made, thereby reducing their risk of recurrent hypoglycaemia. Herein we build a de novo economic model for purposes of incremental analyses to compare, in 2018-19 prices, HS2 against standard care for recurrent hypoglycaemia in the fortnight following the initial attack from the perspective of the UK National Health Service (NHS). We found that per patient NHS costs incurred by people receiving the HS2 intervention over the fortnight following an initial hypoglycaemia average £49.79, and under standard care costs average £40.50. Target patient benefit assessed over that same period finds the probability of no recurrence of hypoglycaemia averaging 42.4% under HS2 and 39.4% under standard care, a 7.6% reduction in relative risk. We find that implementing HS2 will cost the NHS an additional £309.36 per episode of recurrent hypoglycaemia avoided. Contrary to the favourable support offered in Botan et al., we conclude that in its current form the HS2 intervention is not a cost-effective use of NHS resources when compared to standard NHS care in reducing the risk of hypoglycaemia recurring within a fortnight of an initial attack that was resolved at-scene by EMS ambulance clinicians.
Copyright: © 2023 Smith et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The effects of a leaflet-based intervention, 'Hypos can strike twice', on recurrent hypoglycaemic attendances by ambulance services: A non-randomised stepped wedge study.Diabet Med. 2021 Oct;38(10):e14612. doi: 10.1111/dme.14612. Epub 2021 Jun 12. Diabet Med. 2021. PMID: 34053095
-
Prehospital continuous positive airway pressure for acute respiratory failure: the ACUTE feasibility RCT.Health Technol Assess. 2021 Feb;25(7):1-92. doi: 10.3310/hta25070. Health Technol Assess. 2021. PMID: 33538686 Free PMC article. Clinical Trial.
-
Role and prevalence of impaired awareness of hypoglycaemia in ambulance service attendances to people who have had a severe hypoglycaemic emergency: a mixed-methods study.BMJ Open. 2018 Apr 24;8(4):e019522. doi: 10.1136/bmjopen-2017-019522. BMJ Open. 2018. PMID: 29691243 Free PMC article.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.Health Technol Assess. 2005 Feb;9(3):iii-iv, 1-126. doi: 10.3310/hta9030. Health Technol Assess. 2005. PMID: 15694064 Review.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
References
-
- Botan V, Law GR, Laparidou D, Rowan E, Smith MD, Ridyard C, et al.. The effects of a leaflet-based intervention, ‘Hypos can strike twice’, on recurrent hypoglycaemic attendances by ambulance services: A non-randomised stepped wedge study. Diabet Med 2021. Oct;38(10):e14612. doi: 10.1111/dme.14612 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
