

Discriminating Between Compressive Optic Neuropathy With Glaucoma-Like Cupping and Glaucomatous Optic Neuropathy Using OCT and OCTA
- PMID: 36928131
- PMCID: PMC10029766
- DOI: 10.1167/tvst.12.3.11
Discriminating Between Compressive Optic Neuropathy With Glaucoma-Like Cupping and Glaucomatous Optic Neuropathy Using OCT and OCTA
Abstract
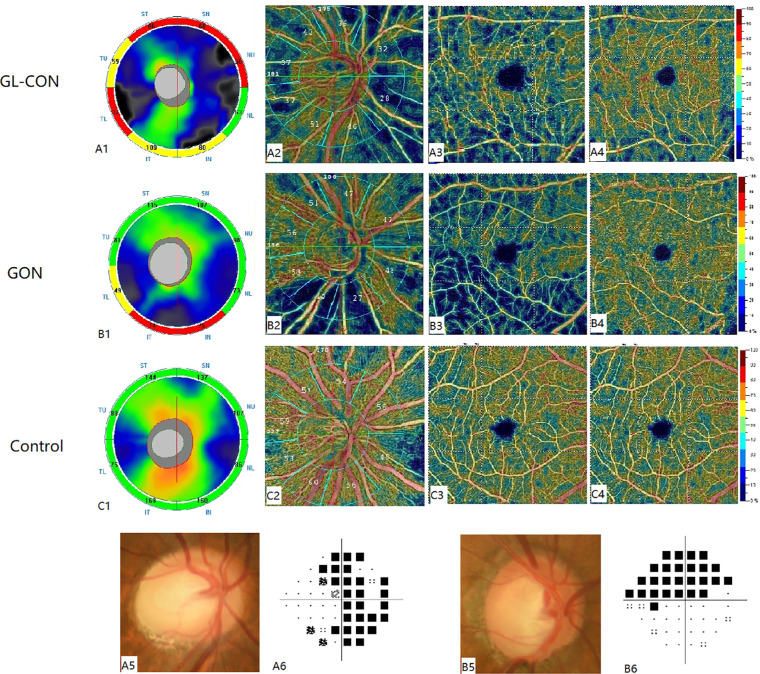
Purpose: To discriminate between compressive optic neuropathy with glaucoma-like cupping (GL-CON) and glaucomatous optic neuropathy (GON) by comparing the peripapillary retinal nerve fiber layer (pRNFL) thickness and retinal microvasculature using optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA).
Methods: In this retrospective cross-sectional study, OCT scans were performed on 28 eyes of GL-CON, 34 eyes of GON, and 41control eyes to determine the pRNFL thickness, ganglion cell complex thickness, and cup/disc ratio. OCTA scans were conducted for 12 eyes of GL-CON, 15 eyes of GON, and 15 control eyes to measure the vessel density of the peripapillary and macular areas. Analysis of covariance was used to perform the comparisons, and the area under the curve was calculated.
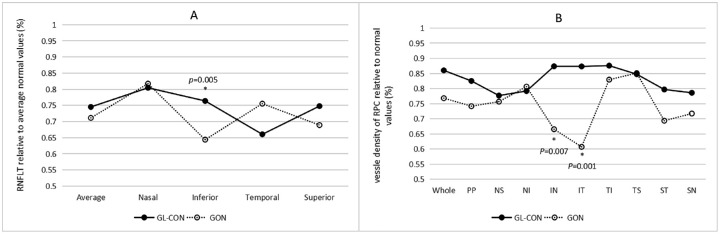
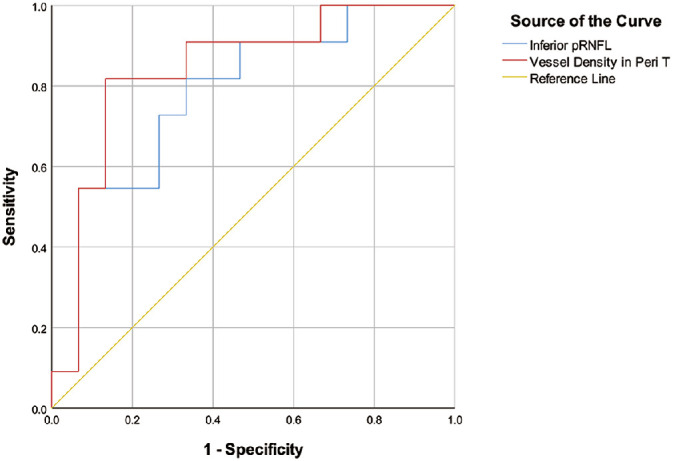
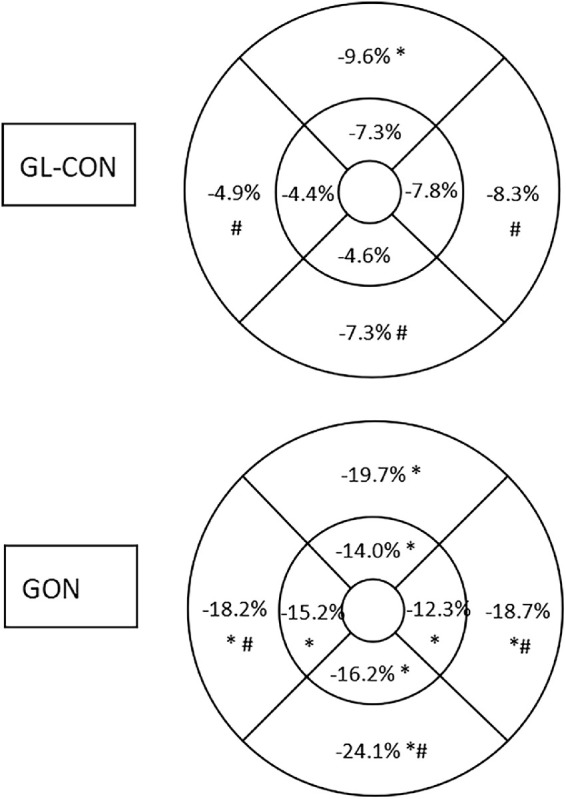
Results: The GON eyes had a significantly thinner pRNFL in the inferior quadrant and greater vertical cup/disc ratio than the GL-CON eyes. In the radial peripapillary capillary segment, the vessel density of the GON in the inferior sectors was significantly lower than in the GL-CON. The superficial macular vessel density in the whole-image, peritemporal, perinasal, and peri-inferior sectors was significantly smaller in the GON group than in the GL-CON group. The best parameter for discriminating between GL-CON and GON was the superficial macular vessel density in the peritemporal sector.
Conclusions: GL-CON eyes showed a characteristic pattern of pRNFL and retinal microvascular changes.
Translational relevance: GL-CON can be effectively distinguished from GON by detecting the alterations in the pRNFL and retinal microvasculature using OCT and OCTA.
Conflict of interest statement
Disclosure:
Figures
References
-
- Greenfield DS, Siatkowski RM, Glaser JS, Schatz NJ, Parrish RK II. The cupped disc: Who needs neuroimaging? Ophthalmology. 1998; 105(10): 1866–1874. - PubMed
-
- Trobe JD, Glaser JS, Cassady J, Herschler J, Anderson DR.. Nonglaucomatous excavation of the optic disc. Arch Ophthalmol. 1980; 98(6): 1046–1050. - PubMed
-
- Andrade TS, Araújo RB, Rocha AADN, Mello LGM, Cunha LP, Monteiro MLR.. Bruch membrane opening minimum rim width and retinal nerve fiber layer helps differentiate compressive optic neuropathy from glaucoma. Am J Ophthalmol. 2022; 234: 156–165. - PubMed
-
- Danesh-Meyer HV, Yap J, Frampton C, Savino PJ.. Differentiation of compressive from glaucomatous optic neuropathy with spectral-domain optical coherence tomography. Ophthalmology. 2014; 121(8): 1516–1523. - PubMed
-
- Leung CKS, Lam AKN, Weinreb RN, et al. .. Diagnostic assessment of glaucoma and non-glaucomatous optic neuropathies via optical texture analysis of the retinal nerve fibre layer. Nat Biomed Eng. 2022; 6(5): 593–604. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
