

Comparison of a machine and deep learning model for automated tumor annotation on digitized whole slide prostate cancer histology
- PMID: 36928230
- PMCID: PMC10019669
- DOI: 10.1371/journal.pone.0278084
Comparison of a machine and deep learning model for automated tumor annotation on digitized whole slide prostate cancer histology
Abstract
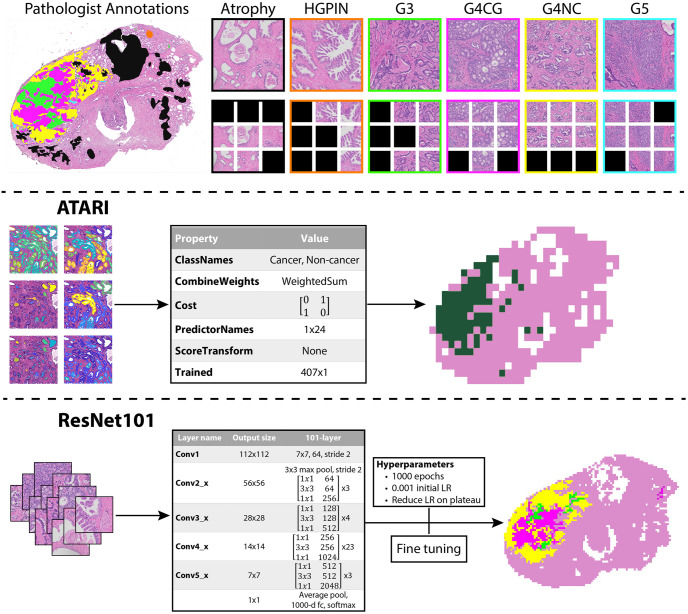
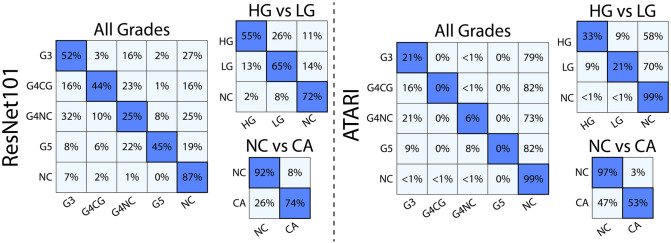
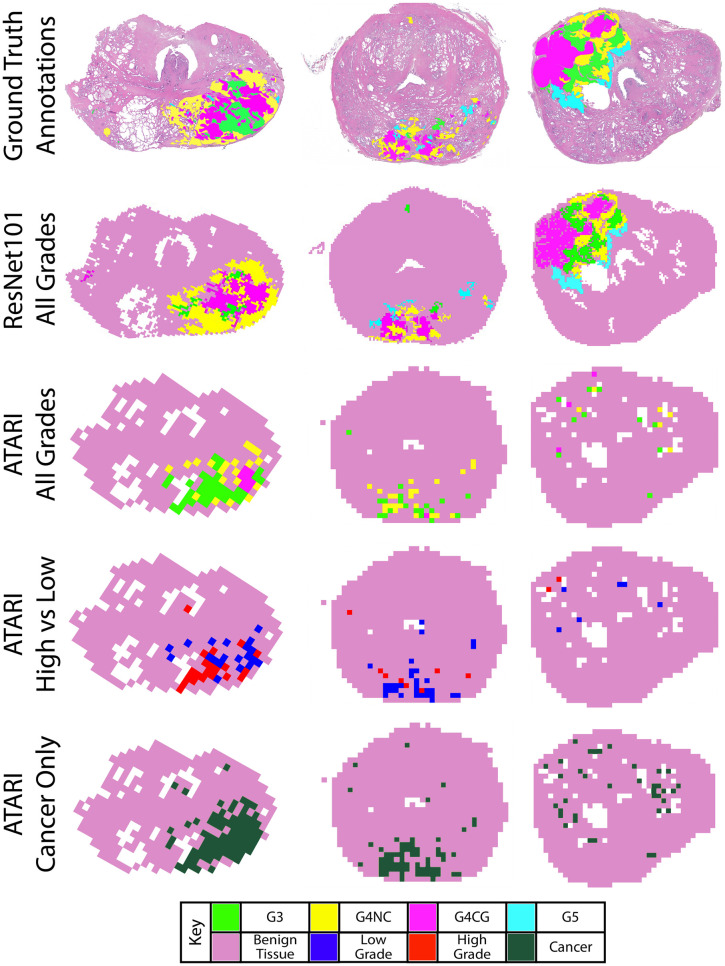
One in eight men will be affected by prostate cancer (PCa) in their lives. While the current clinical standard prognostic marker for PCa is the Gleason score, it is subject to inter-reviewer variability. This study compares two machine learning methods for discriminating between cancerous regions on digitized histology from 47 PCa patients. Whole-slide images were annotated by a GU fellowship-trained pathologist for each Gleason pattern. High-resolution tiles were extracted from annotated and unlabeled tissue. Patients were separated into a training set of 31 patients (Cohort A, n = 9345 tiles) and a testing cohort of 16 patients (Cohort B, n = 4375 tiles). Tiles from Cohort A were used to train a ResNet model, and glands from these tiles were segmented to calculate pathomic features to train a bagged ensemble model to discriminate tumors as (1) cancer and noncancer, (2) high- and low-grade cancer from noncancer, and (3) all Gleason patterns. The outputs of these models were compared to ground-truth pathologist annotations. The ensemble and ResNet models had overall accuracies of 89% and 88%, respectively, at predicting cancer from noncancer. The ResNet model was additionally able to differentiate Gleason patterns on data from Cohort B while the ensemble model was not. Our results suggest that quantitative pathomic features calculated from PCa histology can distinguish regions of cancer; however, texture features captured by deep learning frameworks better differentiate unique Gleason patterns.
Copyright: © 2023 Duenweg et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Srigley JR, Delahunt B, Samaratunga H, Billis A, Cheng L, Clouston D, et al. Controversial issues in Gleason and International Society of Urological Pathology (ISUP) prostate cancer grading: proposed recommendations for international implementation. Pathology. 2019;51(5):463–73. doi: 10.1016/j.pathol.2019.05.001 - DOI - PubMed
