

Toripalimab combined with lenvatinib and GEMOX is a promising regimen as first-line treatment for advanced intrahepatic cholangiocarcinoma: a single-center, single-arm, phase 2 study
- PMID: 36928584
- PMCID: PMC10020443
- DOI: 10.1038/s41392-023-01317-7
Toripalimab combined with lenvatinib and GEMOX is a promising regimen as first-line treatment for advanced intrahepatic cholangiocarcinoma: a single-center, single-arm, phase 2 study
Abstract
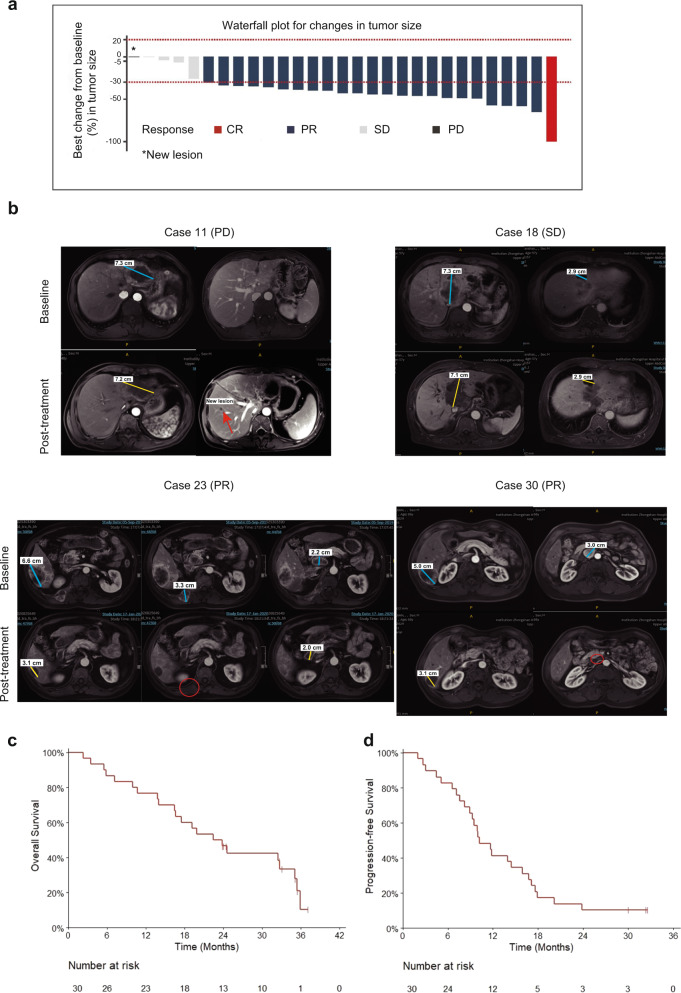
Advanced intrahepatic cholangiocarcinoma (ICC) has a dismal prognosis. Here, we report the efficacy and safety of combining toripalimab, lenvatinib, and gemcitabine plus oxaliplatin (GEMOX) as first-line therapy for advanced ICC. Thirty patients with pathologically confirmed advanced ICC received intravenous gemcitabine (1 g/m2) on Days 1 and 8 and oxaliplatin (85 mg/m2) Q3W for six cycles along with intravenous toripalimab (240 mg) Q3W and oral lenvatinib (8 mg) once daily for one year. The expression of programmed death-ligand 1 (PD-L1) and genetic status was investigated in paraffin-embedded tissues using immunohistochemistry and whole-exome sequencing (WES) analysis. The primary endpoint was the objective response rate (ORR). Secondary outcomes included safety, overall survival (OS), progression-free survival (PFS), disease control rate (DCR) and duration of response (DoR). As of July 1, 2022, the median follow-up time was 23.5 months, and the ORR was 80%. Twenty-three patients achieved partial response, and one achieved complete response. Patients (21/30) with DNA damage response (DDR)-related gene mutations showed a higher ORR, while patients (14/30) with tumor area positivity ≥1 (PD-L1 staining) showed a trend of high ORR, but without significant difference. The median OS, PFS, and DoR were 22.5, 10.2, and 11.0 months, respectively. The DCR was 93.3%. Further, 56.7% of patients experienced manageable grade ≥3 adverse events (AEs), commonly neutropenia (40.0%) and leukocytopenia (23.3%). In conclusion, toripalimab plus lenvatinib and GEMOX are promising first-line regimens for the treatment of advanced ICC. A phase-III, multicenter, double-blinded, randomized study to validate our findings was approved by the National Medical Products Administration (NMPA, No. 2021LP01825).Trial registration Clinical trials: NCT03951597.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
