

Cystic Lesions of the Jaws: The Top 10 Differential Diagnoses to Ponder
- PMID: 36928736
- PMCID: PMC10063769
- DOI: 10.1007/s12105-023-01525-1
Cystic Lesions of the Jaws: The Top 10 Differential Diagnoses to Ponder
Abstract
Background: Cystic lesions of the gnathic bones present challenges in differential diagnosis. This category includes a smorgasbord of odontogenic and non-odontogenic entities that may be reactive or neoplastic in nature. While most cystic jaw lesions are benign, variability in biologic behavior makes distinction between these entities absolutely crucial.
Methods: Review.
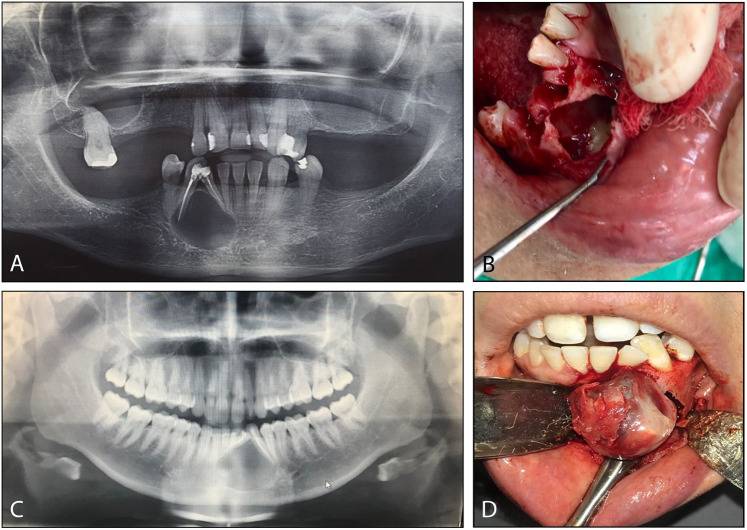
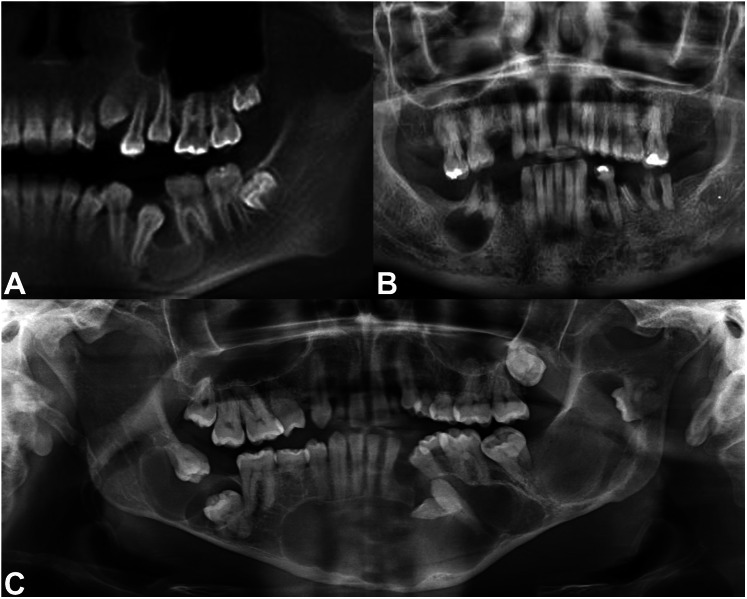
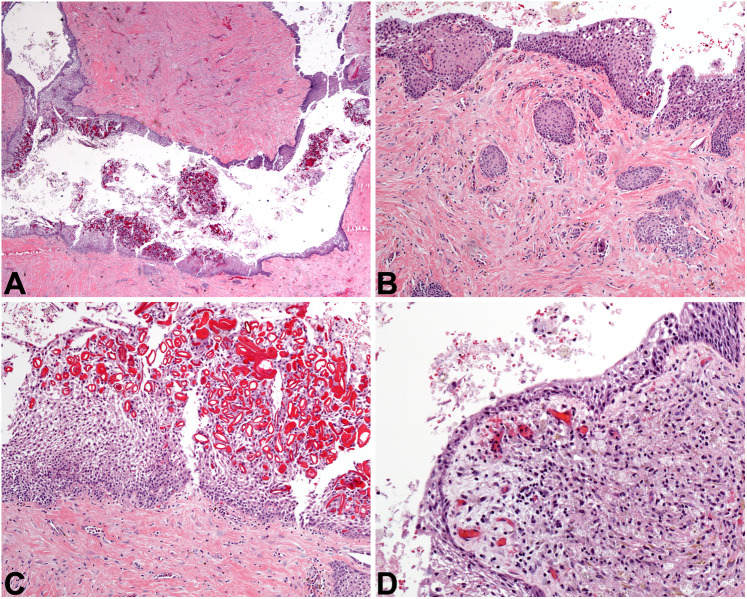
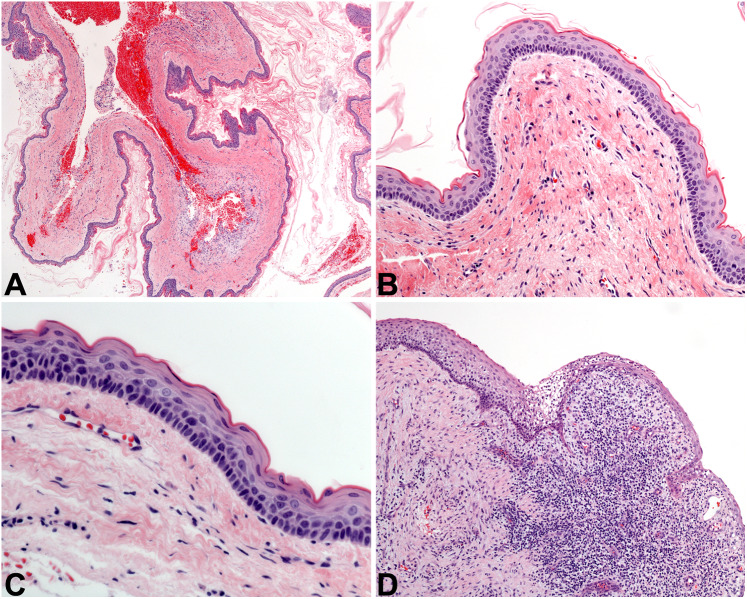
Results: Two clinical cases are presented in parallel and are followed by an illustrated discussion of the ten most likely differential diagnoses that should be considered when confronted with a cystic jaw lesion. Strong emphasis is placed on the histologic differences between these entities, empowering readers to diagnose them with confidence. Perhaps even more importantly, the more common diagnostic pitfalls in gnathic pathology are discussed, recognizing that a definitive diagnosis cannot be rendered in every situation. The histologic diagnoses for the two clinical cases are finally revealed.
Conclusion: Cystic lesions of the maxilla and mandible may be odontogenic or non-odontogenic. The most common cystic lesions are the reactive periapical cyst, and the dentigerous cyst (which is developmental in nature). It is important to note that cystic neoplasms also occur in the jaws, and that the presence of inflammation may obscure the diagnostic histologic features of lesions like odontogenic keratocyst and unicystic ameloblastoma. Ancillary testing is of limited diagnostic value in most scenarios. However, both clinical and radiographic information (such as the location, size, duration, associated symptoms, and morphology of the lesion in its natural habitat) are significantly useful.
Keywords: Cyst; Differential diagnosis; Jaws; Mandible; Maxilla; Odontogenic; Review.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
