

Multiomic neuropathology improves diagnostic accuracy in pediatric neuro-oncology
- PMID: 36928815
- PMCID: PMC10115638
- DOI: 10.1038/s41591-023-02255-1
Multiomic neuropathology improves diagnostic accuracy in pediatric neuro-oncology
Erratum in
-
Author Correction: Multiomic neuropathology improves diagnostic accuracy in pediatric neuro-oncology.Nat Med. 2024 Jan;30(1):306. doi: 10.1038/s41591-023-02652-6. Nat Med. 2024. PMID: 37875569 Free PMC article. No abstract available.
Abstract
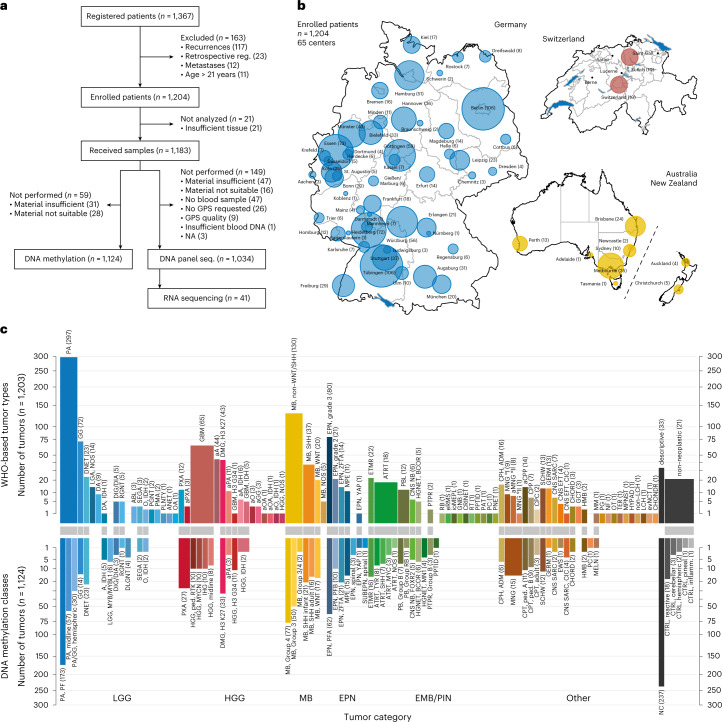
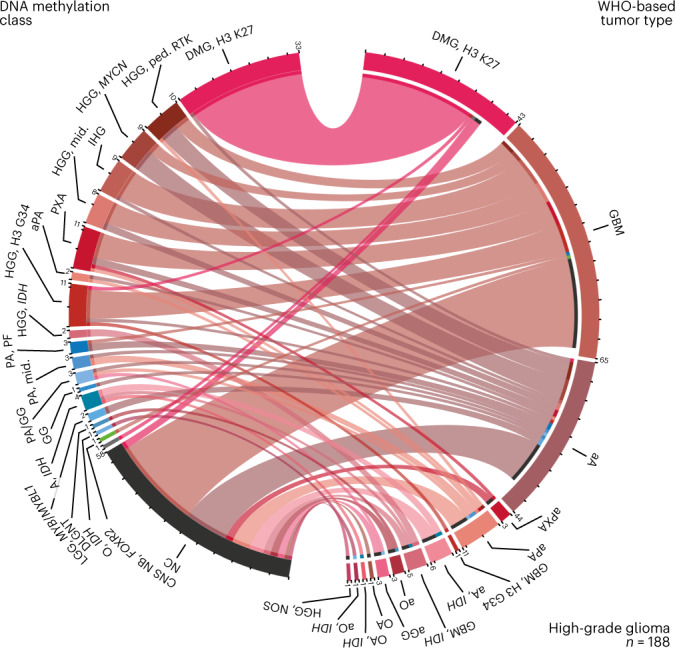
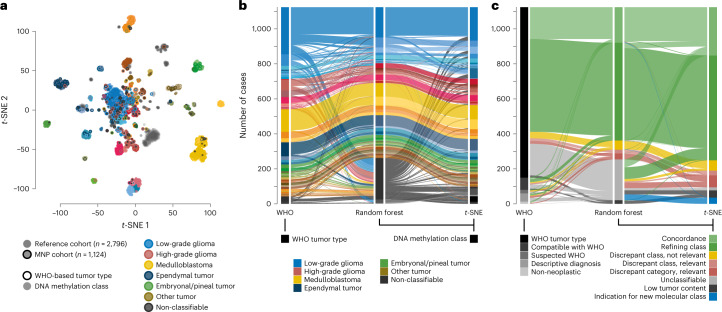
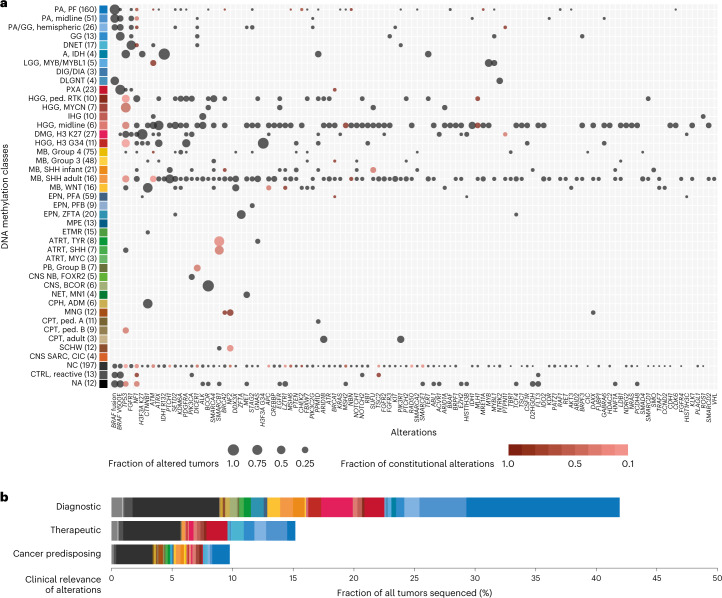
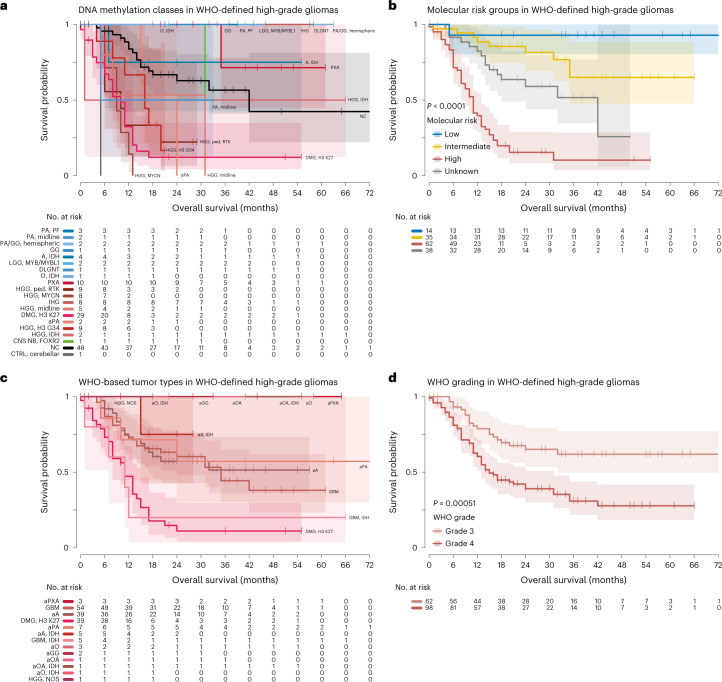
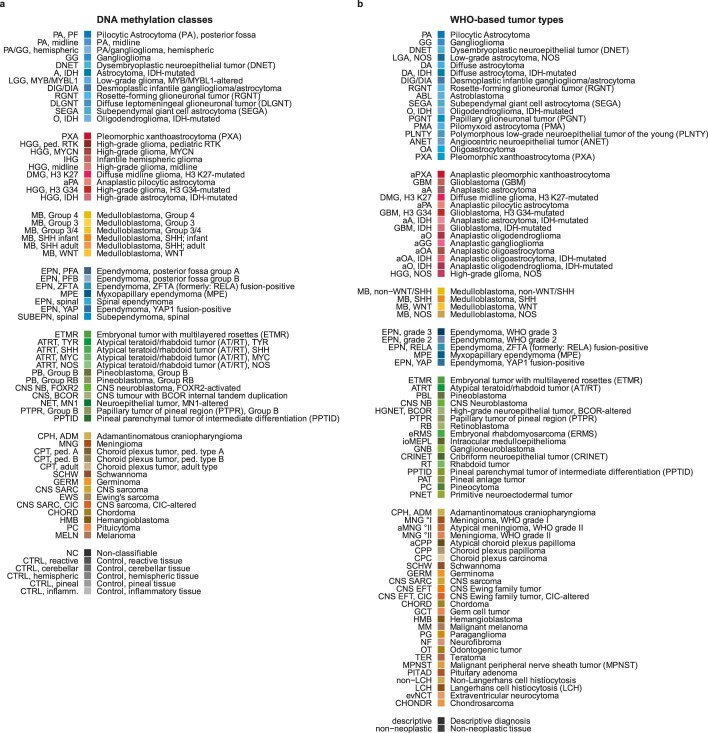
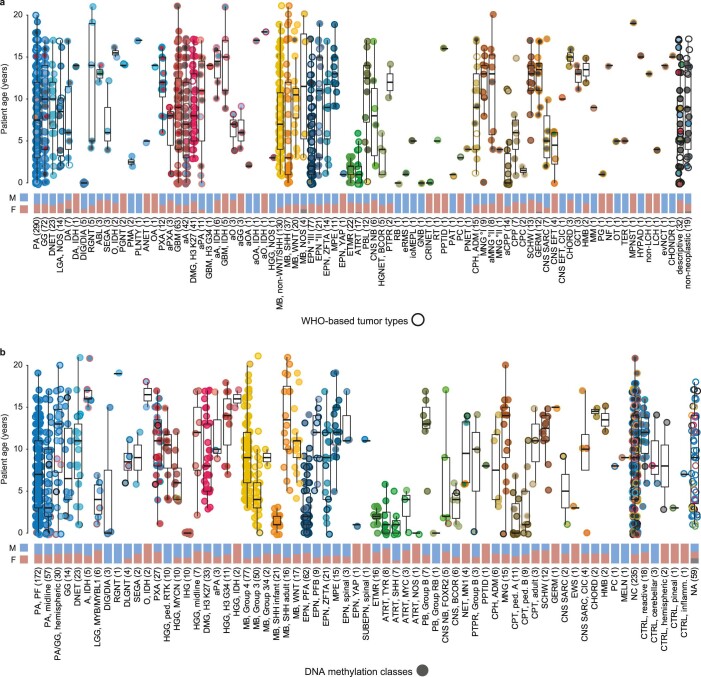
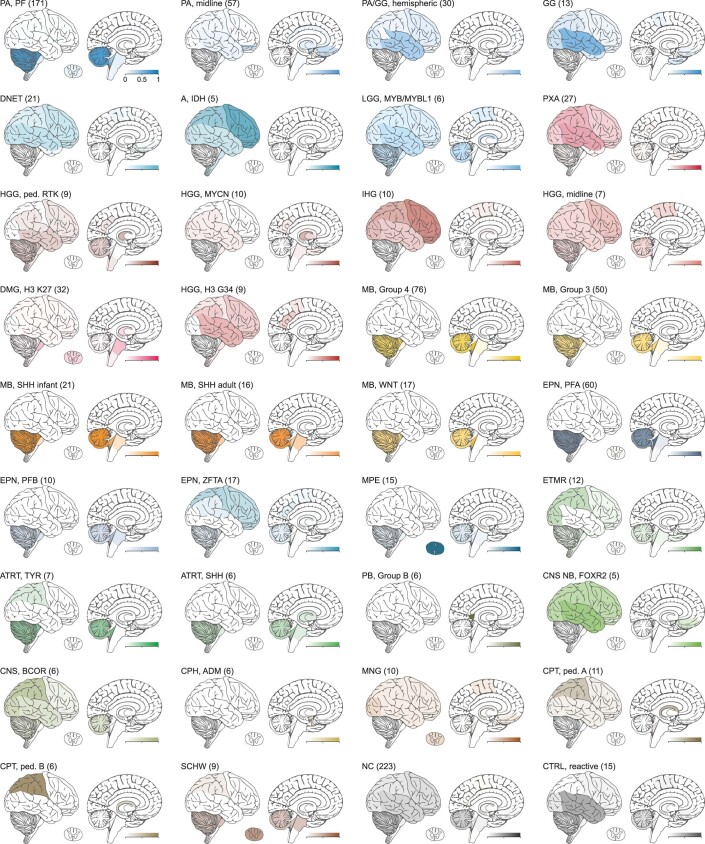
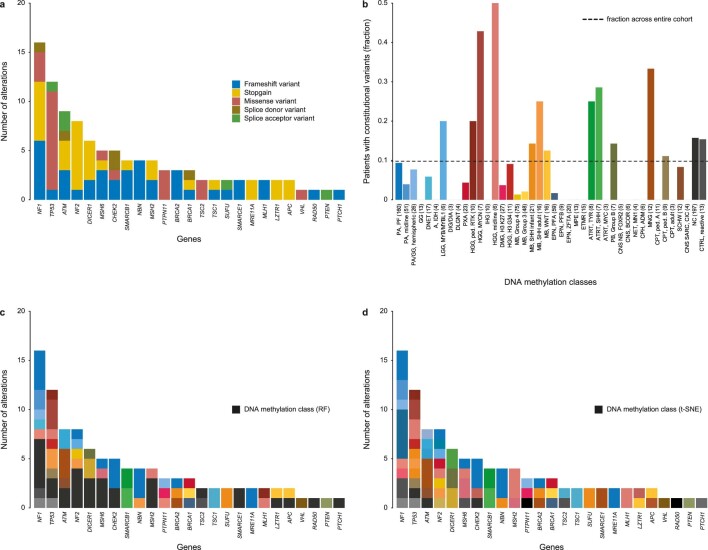
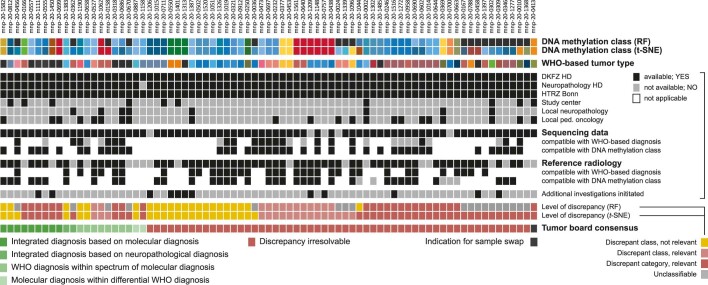
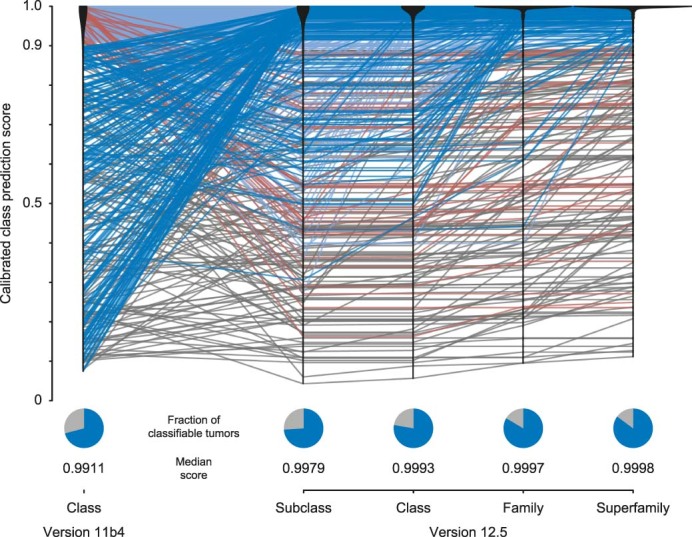
The large diversity of central nervous system (CNS) tumor types in children and adolescents results in disparate patient outcomes and renders accurate diagnosis challenging. In this study, we prospectively integrated DNA methylation profiling and targeted gene panel sequencing with blinded neuropathological reference diagnostics for a population-based cohort of more than 1,200 newly diagnosed pediatric patients with CNS tumors, to assess their utility in routine neuropathology. We show that the multi-omic integration increased diagnostic accuracy in a substantial proportion of patients through annotation to a refining DNA methylation class (50%), detection of diagnostic or therapeutically relevant genetic alterations (47%) or identification of cancer predisposition syndromes (10%). Discrepant results by neuropathological WHO-based and DNA methylation-based classification (30%) were enriched in histological high-grade gliomas, implicating relevance for current clinical patient management in 5% of all patients. Follow-up (median 2.5 years) suggests improved survival for patients with histological high-grade gliomas displaying lower-grade molecular profiles. These results provide preliminary evidence of the utility of integrating multi-omics in neuropathology for pediatric neuro-oncology.
© 2023. The Author(s).
Conflict of interest statement
D.C., M.S., D. Schrimpf, A.v.D., F.S., S.M.P. and D.T.W.J. are shareholders in and co-founders of Heidelberg Epignostix GmbH. All other authors declare no competing interests.
Figures
Comment in
-
Accurate diagnosis of pediatric brain cancers.Nat Med. 2023 Apr;29(4):787-788. doi: 10.1038/s41591-023-02254-2. Nat Med. 2023. PMID: 36932243 No abstract available.
References
-
- Louis, D.N., Ohgaki, H., Wiestler, O.D. & Cavenee, W.K. WHO Classification of Tumours of the Central Nervous System. Revised 4th ed (WHO Press, 2016).
-
- WHO Classification of Tumours Editorial Board. Central Nervous System Tumours. WHO Classification of Tumours, 5th ed, vol 6. https://publications.iarc.fr/601 (International Agency for Research on Cancer, 2021).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
