

Clinical features and prognostic factors in adults with viral meningitis
- PMID: 36929167
- PMCID: PMC10473559
- DOI: 10.1093/brain/awad089
Clinical features and prognostic factors in adults with viral meningitis
Abstract
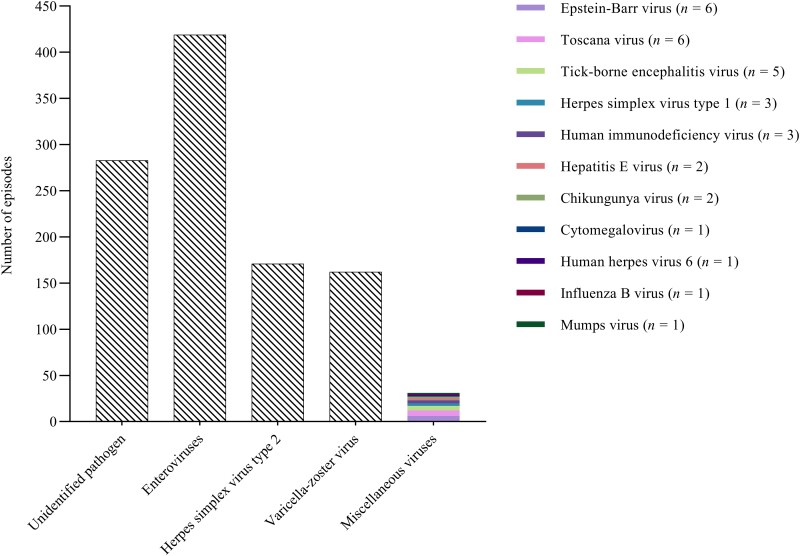
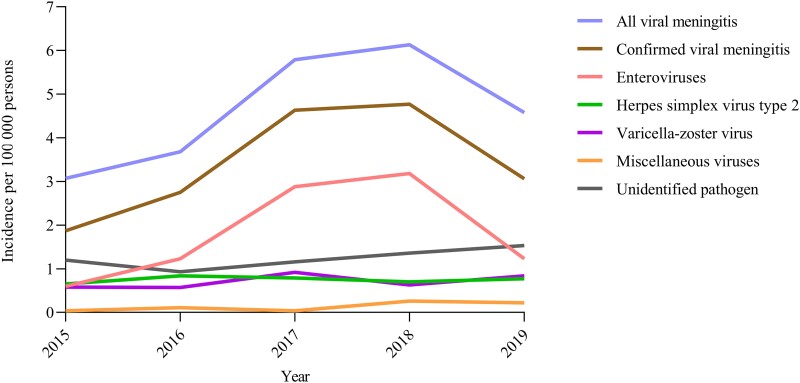
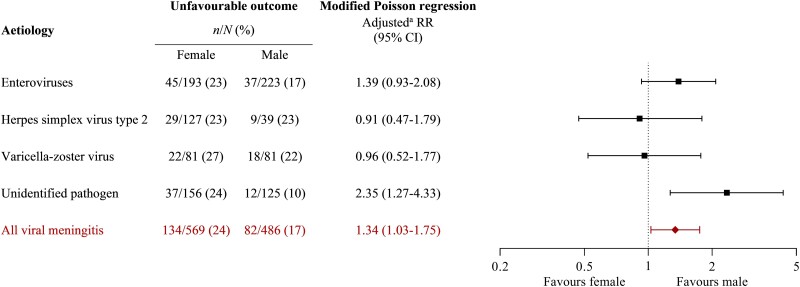
Clinical features applicable to the entire spectrum of viral meningitis are limited, and prognostic factors for adverse outcomes are undetermined. This nationwide population-based prospective cohort study included all adults with presumed and microbiologically confirmed viral meningitis in Denmark from 2015 until 2020. Prognostic factors for an unfavourable outcome (Glasgow Outcome Scale score of 1-4) 30 days after discharge were examined by modified Poisson regression. In total, 1066 episodes of viral meningitis were included, yielding a mean annual incidence of 4.7 episodes per 100 000 persons. Pathogens were enteroviruses in 419/1066 (39%), herpes simplex virus type 2 in 171/1066 (16%), varicella-zoster virus in 162/1066 (15%), miscellaneous viruses in 31/1066 (3%) and remained unidentified in 283/1066 (27%). The median age was 33 years (IQR 27-44), and 576/1066 (54%) were females. In herpes simplex virus type 2 meningitis, 131/171 (77%) were females. Immunosuppression [32/162 (20%)] and shingles [90/149 (60%)] were frequent in varicella-zoster virus meningitis. The triad of headache, neck stiffness and hyperacusis or photophobia was present in 264/960 (28%). The median time until lumbar puncture was 3.0 h (IQR 1.3-7.1), and the median CSF leucocyte count was 160 cells/µl (IQR 60-358). The outcome was unfavourable in 216/1055 (20%) 30 days after discharge. Using unidentified pathogen as the reference, the adjusted relative risk of an unfavourable outcome was 1.34 (95% CI 0.95-1.88) for enteroviruses, 1.55 (95% CI 1.00-2.41) for herpes simplex virus type 2, 1.51 (95% CI 0.98-2.33) for varicella-zoster virus and 1.37 (95% CI 0.61-3.05) for miscellaneous viruses. The adjusted relative risk of an unfavourable outcome was 1.34 (95% CI 1.03-1.75) for females. Timing of acyclovir or valacyclovir was not associated with the outcome in meningitis caused by herpes simplex virus type 2 or varicella-zoster virus. In summary, the outcome of viral meningitis was similar among patients with different aetiologies, including those with presumed viral meningitis but without an identified pathogen. Females had an increased risk of an unfavourable outcome. Early antiviral treatment was not associated with an improved outcome in meningitis caused by herpes simplex virus type 2 or varicella-zoster virus.
Keywords: aseptic meningitis; herpesviridae; tick-borne encephalitis; toscana virus; virology.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures
References
-
- Kupila L, Vuorinen T, Marttila RJ, Kotilainen P. Etiology of aseptic meningitis and encephalitis in an adult population. Neurology. 2006;66:6. - PubMed
-
- Franzen-Röhl E, Larsson K, Skoog E, et al. High diagnostic yield by CSF-PCR for entero- and herpes simplex viruses and TBEV serology in adults with acute aseptic meningitis in Stockholm. Scand J Infect Dis. 2008;40:914–921. - PubMed
-
- de Ory F, Avellón A, Echevarría Je, et al. Viral infections of the central nervous system in Spain: A prospective study. J Med Virol. 2013;85:554–562. - PubMed
-
- Calleri G, Libanore V, Corcione S, Rosa FGD, Caramello P. A retrospective study of viral central nervous system infections: Relationship amongst aetiology, clinical course and outcome. Infection. 2017;45:227–231. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
