

Readmission Rates and Episode Costs for Alzheimer Disease and Related Dementias Across Hospitals in a Statewide Collaborative
- PMID: 36929401
- PMCID: PMC10020873
- DOI: 10.1001/jamanetworkopen.2023.2109
Readmission Rates and Episode Costs for Alzheimer Disease and Related Dementias Across Hospitals in a Statewide Collaborative
Abstract
Importance: There has been a paucity of research examining the risk and cost of readmission among patients with Alzheimer disease and related dementias (ADRD) after a planned hospitalization for a broad set of medical and surgical procedures.
Objective: To examine 30-day readmission rates and episode costs, including readmission costs, for patients with ADRD compared with their counterparts without ADRD across Michigan hospitals.
Design, setting, and participants: This retrospective cohort study used 2012 to 2017 Michigan Value Collaborative data across different medical and surgical services stratified by ADRD diagnosis. A total of 66 676 admission episodes of care that occurred between January 1, 2012, and June 31, 2017, were identified for patients with ADRD using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic codes for ADRD, along with 656 235 admission episodes in patients without ADRD. Using a generalized linear model framework, this study risk adjusted, price standardized, and performed episode payment winsorization. Payments were risk adjusted for age, sex, Hierarchical Condition Categories, insurance type, and prior 6-month payments. Selection bias was accounted for using multivariable logistic regression with propensity score matching without replacement using calipers. Data analysis was performed from January to December 2019.
Exposure: Presence of ADRD.
Main outcomes and measures: Main outcomes were 30-day readmission rate at the patient and county levels, 30-day readmission cost, and 30-day total episode cost across 28 medical and surgical services.
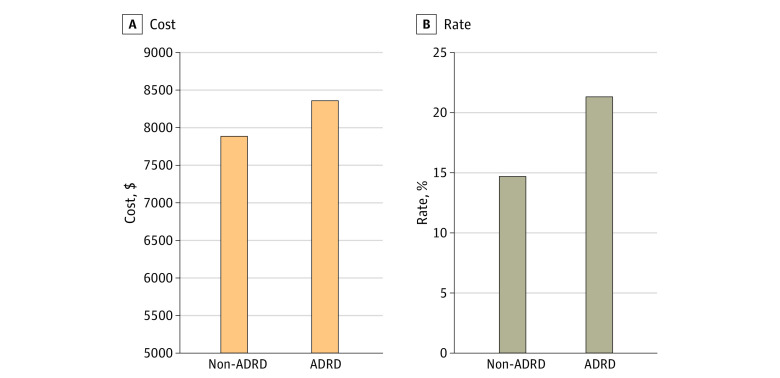
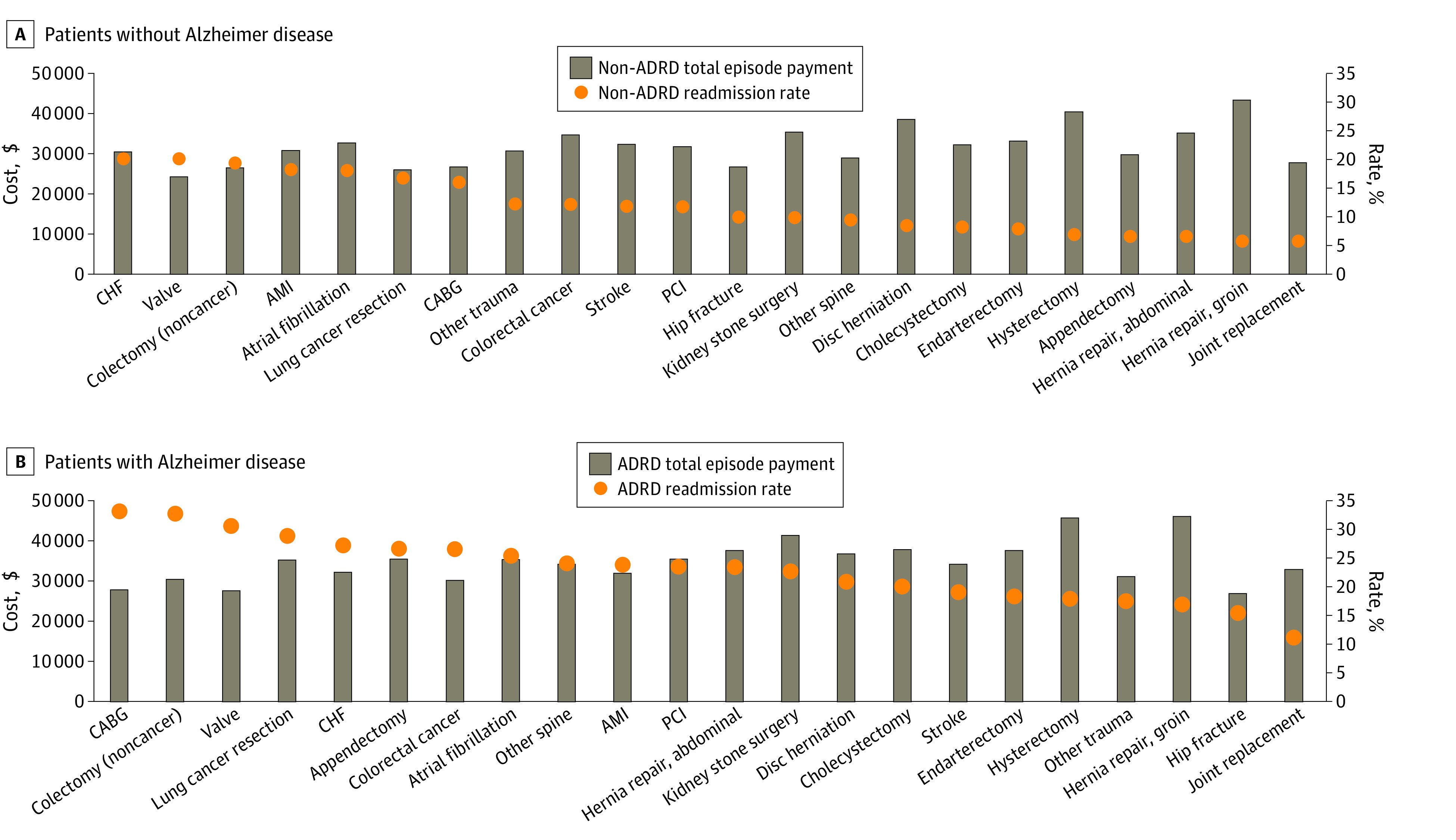
Results: The study included 722 911 hospitalization episodes, of which 66 676 were related to patients with ADRD (mean [SD] age, 83.4 [8.6] years; 42 439 [63.6%] female) and 656 235 were related to patients without ADRD (mean [SD] age, 66.0 [15.4] years; 351 246 [53.5%] female). After propensity score matching, 58 629 hospitalization episodes were included for each group. Readmission rates were 21.5% (95% CI, 21.2%-21.8%) for patients with ADRD and 14.7% (95% CI, 14.4%-15.0%) for patients without ADRD (difference, 6.75 percentage points; 95% CI, 6.31-7.19 percentage points). Cost of 30-day readmission was $467 higher (95% CI of difference, $289-$645) among patients with ADRD ($8378; 95% CI, $8263-$8494) than those without ($7912; 95% CI, $7776-$8047). Across all 28 service lines examined, total 30-day episode costs were $2794 higher for patients with ADRD vs patients without ADRD ($22 371 vs $19 578; 95% CI of difference, $2668-$2919).
Conclusions and relevance: In this cohort study, patients with ADRD had higher readmission rates and overall readmission and episode costs than their counterparts without ADRD. Hospitals may need to be better equipped to care for patients with ADRD, especially in the postdischarge period. Considering that any type of hospitalization may put patients with ADRD at a high risk of 30-day readmission, judicious preoperative assessment, postoperative discharge, and care planning are strongly advised for this vulnerable patient population.
Conflict of interest statement
Figures
Similar articles
-
Costs and Consequences of Early Hospital Discharge After Major Inpatient Surgery in Older Adults.JAMA Surg. 2017 May 17;152(5):e170123. doi: 10.1001/jamasurg.2017.0123. Epub 2017 May 17. JAMA Surg. 2017. PMID: 28329352 Free PMC article.
-
Drivers of Payment Variation in 90-Day Coronary Artery Bypass Grafting Episodes.JAMA Surg. 2018 Jan 1;153(1):14-19. doi: 10.1001/jamasurg.2017.2881. JAMA Surg. 2018. PMID: 28832865 Free PMC article.
-
Association of Medicare bundled payment model with joint replacement care for people with dementia.J Am Geriatr Soc. 2022 Sep;70(9):2571-2581. doi: 10.1111/jgs.17836. Epub 2022 May 30. J Am Geriatr Soc. 2022. PMID: 35635471 Free PMC article.
-
Optimizing coding and reimbursement to improve management of Alzheimer's disease and related dementias.J Am Geriatr Soc. 2002 Nov;50(11):1871-8. doi: 10.1046/j.1532-5415.2002.50519.x. J Am Geriatr Soc. 2002. PMID: 12410910 Review.
-
Observational studies in Alzheimer disease: bridging preclinical studies and clinical trials.Nat Rev Neurol. 2022 Dec;18(12):747-757. doi: 10.1038/s41582-022-00733-7. Epub 2022 Oct 31. Nat Rev Neurol. 2022. PMID: 36316487 Free PMC article. Review.
Cited by
-
Racial/Ethnic Disparities in Hospital Readmission and Frequent Hospitalizations Among Medicare Beneficiaries With Alzheimer's Disease and Related Dementia: Traditional Medicare Versus Medicare Advantage.J Gerontol B Psychol Sci Soc Sci. 2024 Jul 1;79(7):gbae078. doi: 10.1093/geronb/gbae078. J Gerontol B Psychol Sci Soc Sci. 2024. PMID: 38733162 Free PMC article.
-
Association of Alzheimer's Disease and Related Dementias (ADRD) With Days at Home Among Medicare Beneficiaries After a Heart Failure Hospitalization.Circ Cardiovasc Qual Outcomes. 2025 Jun;18(6):e011246. doi: 10.1161/CIRCOUTCOMES.124.011246. Epub 2025 Apr 30. Circ Cardiovasc Qual Outcomes. 2025. PMID: 40304047
-
CEDART Study: protocol for a non-randomized feasibility study.Res Sq [Preprint]. 2025 May 13:rs.3.rs-6378596. doi: 10.21203/rs.3.rs-6378596/v1. Res Sq. 2025. PMID: 40470215 Free PMC article. Preprint.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
