

Improving health outcomes of people with diabetes: target setting for the WHO Global Diabetes Compact
- PMID: 36931289
- PMCID: PMC10420388
- DOI: 10.1016/S0140-6736(23)00001-6
Improving health outcomes of people with diabetes: target setting for the WHO Global Diabetes Compact
Abstract
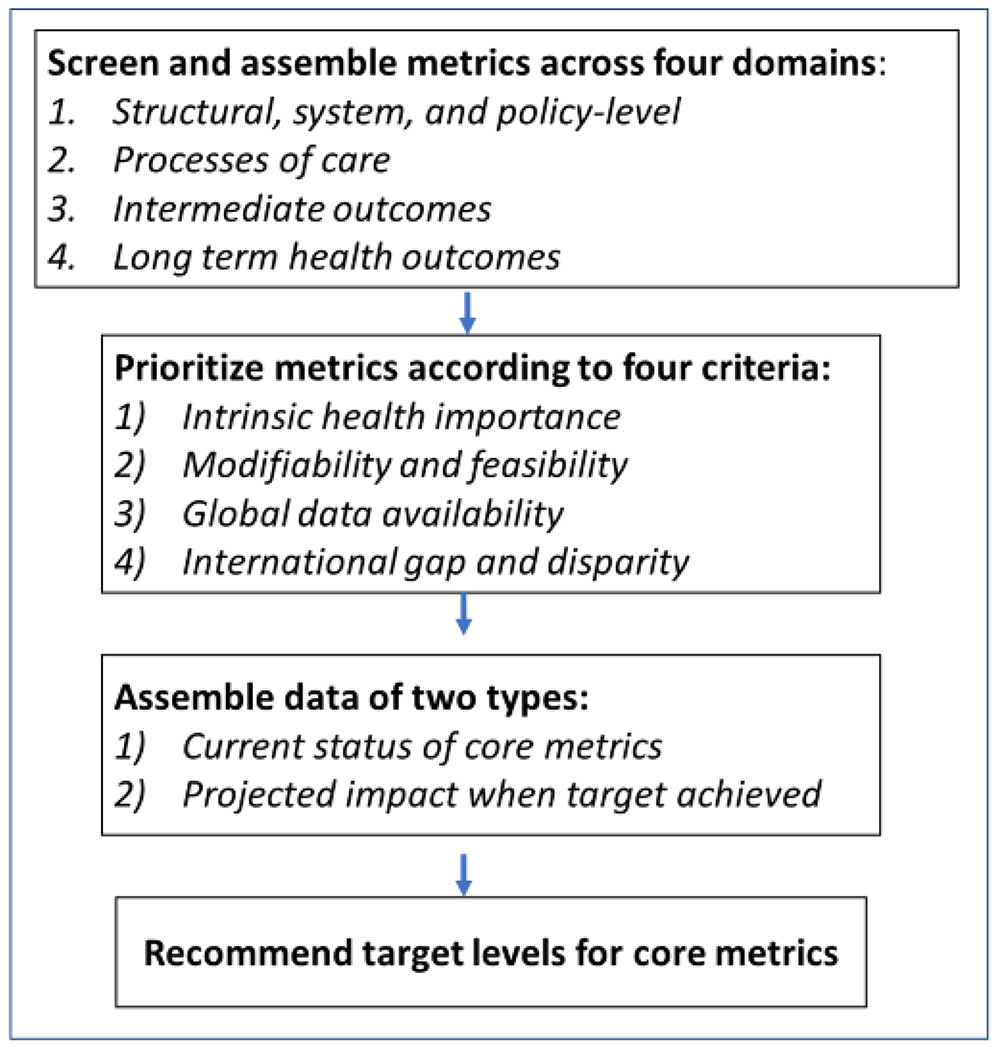
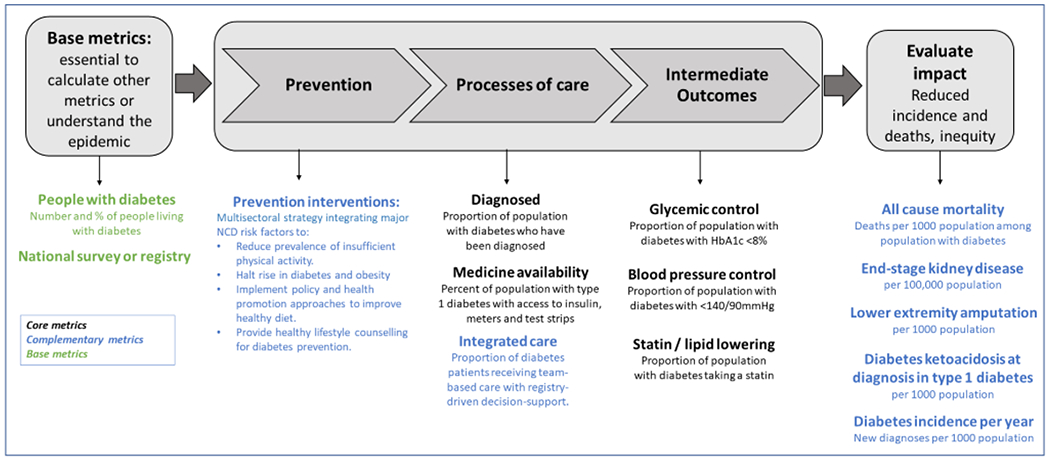
The Global Diabetes Compact is a WHO-driven initiative uniting stakeholders around goals of reducing diabetes risk and ensuring that people with diabetes have equitable access to comprehensive, affordable care and prevention. In this report we describe the development and scientific basis for key health metrics, coverage, and treatment targets accompanying the Compact. We considered metrics across four domains: factors at a structural, system, or policy level; processes of care; behaviours and biomarkers such as glycated haemoglobin (HbA1c); and health events and outcomes; and three risk tiers (diagnosed diabetes, high risk, or whole population), and reviewed and prioritised them according to their health importance, modifiability, data availability, and global inequality. We reviewed the global distribution of each metric to set targets for future attainment. This process led to five core national metrics and target levels for UN member states: (1) of all people with diabetes, at least 80% have been clinically diagnosed; and, for people with diagnosed diabetes, (2) 80% have HbA1c concentrations below 8·0% (63·9 mmol/mol); (3) 80% have blood pressure lower than 140/90 mm Hg; (4) at least 60% of people 40 years or older are receiving therapy with statins; and (5) each person with type 1 diabetes has continuous access to insulin, blood glucose meters, and test strips. We also propose several complementary metrics that currently have limited global coverage, but warrant scale-up in population-based surveillance systems. These include estimation of cause-specific mortality, and incidence of end-stage kidney disease, lower-extremity amputations, and incidence of diabetes. Primary prevention of diabetes and integrated care to prevent long-term complications remain important areas for the development of new metrics and targets. These metrics and targets are intended to drive multisectoral action applied to individuals, health systems, policies, and national health-care access to achieve the goals of the Global Diabetes Compact. Although ambitious, their achievement can result in broad health benefits for people with diabetes.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests WHO provided financial support and two affiliated advisers contributed as authors. EWG and JB report receiving consultation funding from WHO related to this work. EWG also receives funding from UK Royal Society and Science Foundation Ireland. Authors report the following funding unrelated to this study and report: MKA reports funding from Merck, Bayer, and Eli Lilly; RM reports consulting fees from Novo Nordisk, Eli Lilly, Boeheringer Ingelheim, Sanofi, and AstraZeneca; L-LL reports grants or honoraria from AstraZeneca, Boeheringer Ingelheim, Abbott, Merck Sharp & Dohme, Sanofi, Servier, Zuellig Pharma, and Pfizer; JPS reports funding from Novo Nordisk and Pfizer; JES reports funding from AstraZeneca, Sanofi, Novo Nordisk, MSD, Eli Lilly, and Pfizer, Mylan, Sanofi, Boehringer Ingelheim, and Zuellig Pharma. All other authors declare no competing interests.
Figures
Comment in
-
Recommendations from 'Improving health outcomes of people with diabetes: Target setting for the WHO Global Diabetes Compact' for the Indian context: Laudable but are they achievable?Natl Med J India. 2023 Sep-Oct;36(5):281-282. doi: 10.25259/NMJI_713_2023. Natl Med J India. 2023. PMID: 38759989 No abstract available.
References
-
- Federation ID. IDF Diabetes Atlas. 2021. www.diabetesatlas.org.
-
- Chan JCN, Lim LL, Wareham NJ, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. Lancet 2021; 396(10267): 2019–82. - PubMed
-
- Williams R, Karuranga S, Malanda B, et al. Global and regional estimates and projections of diabetes-related health expenditure: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2020; 162: 108072. - PubMed
-
- Bommer C, Heesemann E, Sagalova V, et al. The global economic burden of diabetes in adults aged 20-79 years: a cost-of-illness study. Lancet Diabetes Endocrinol 2017; 5(6): 423–30. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
