

The accumulated oxygen deficit as an indicator of the ischemic retinal insult
- PMID: 36931487
- PMCID: PMC10133208
- DOI: 10.1016/j.exer.2023.109439
The accumulated oxygen deficit as an indicator of the ischemic retinal insult
Abstract
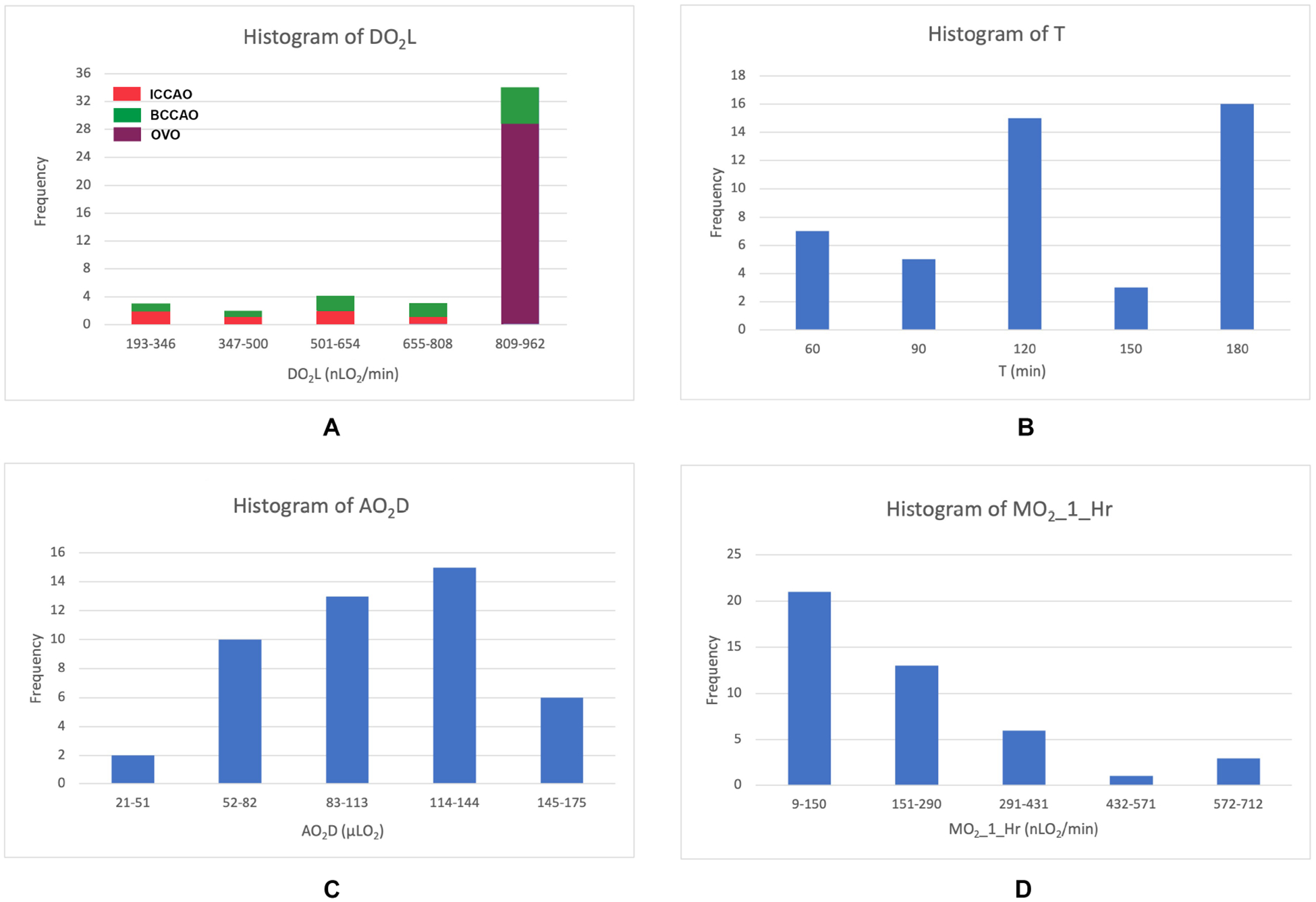
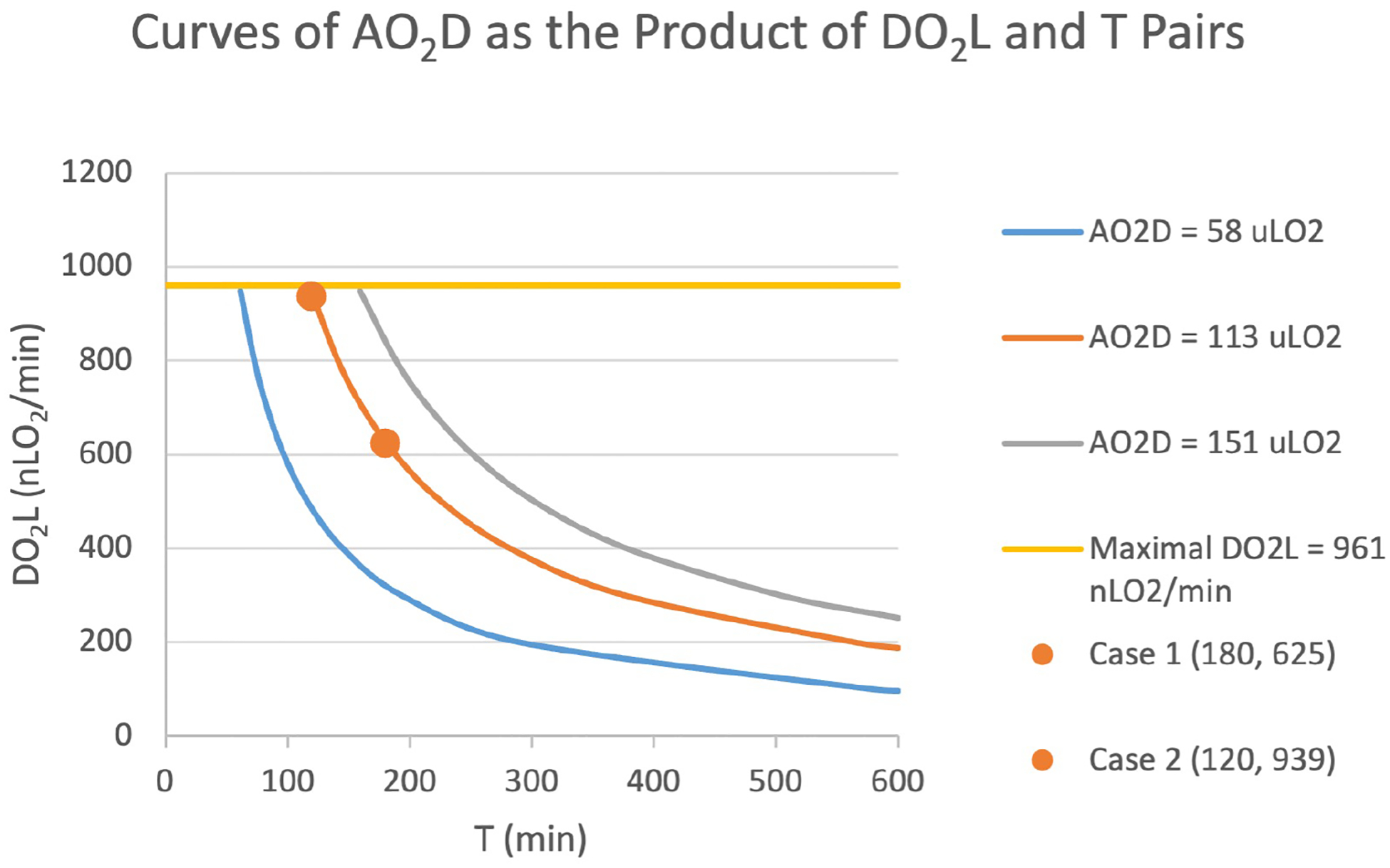
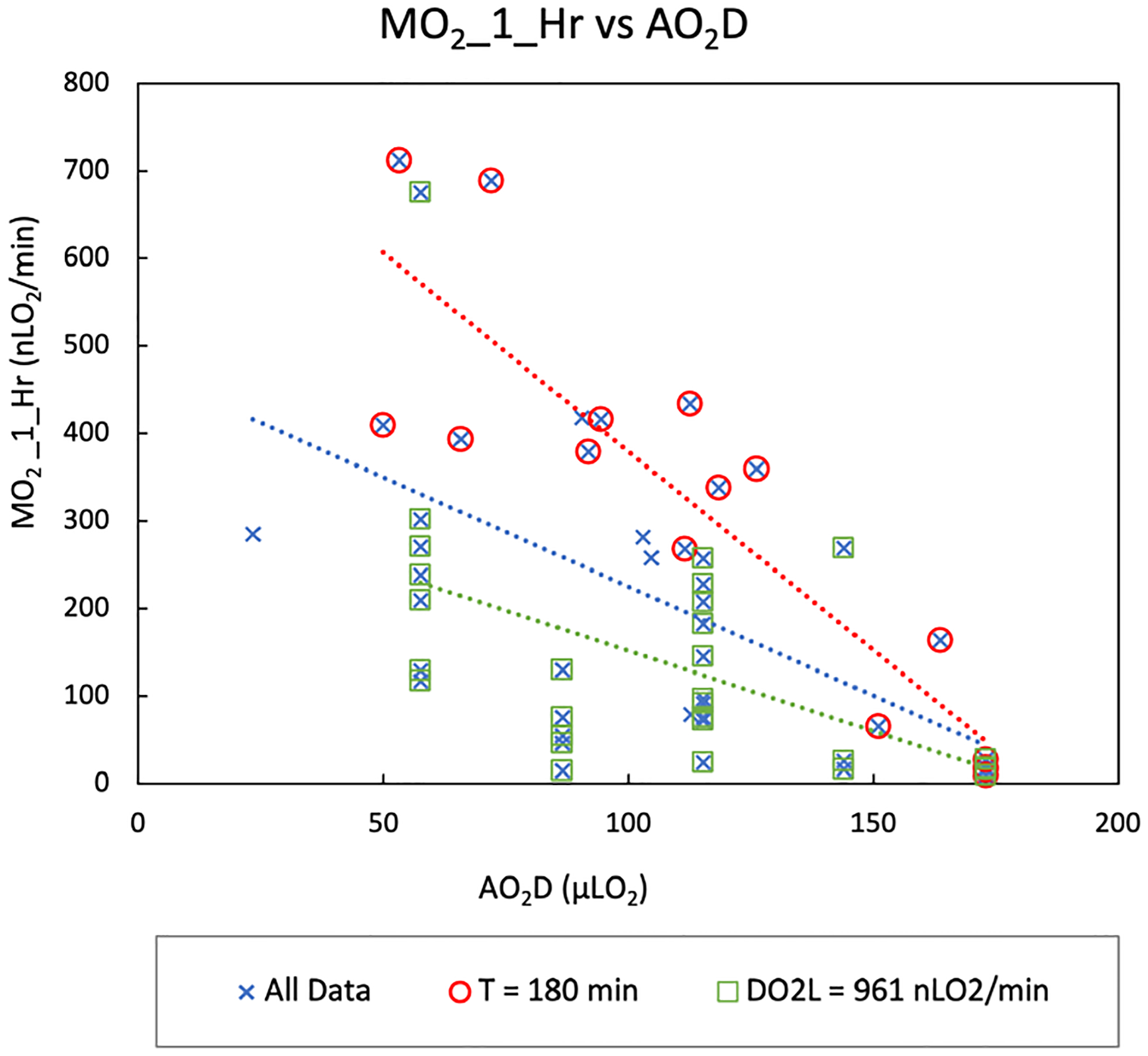
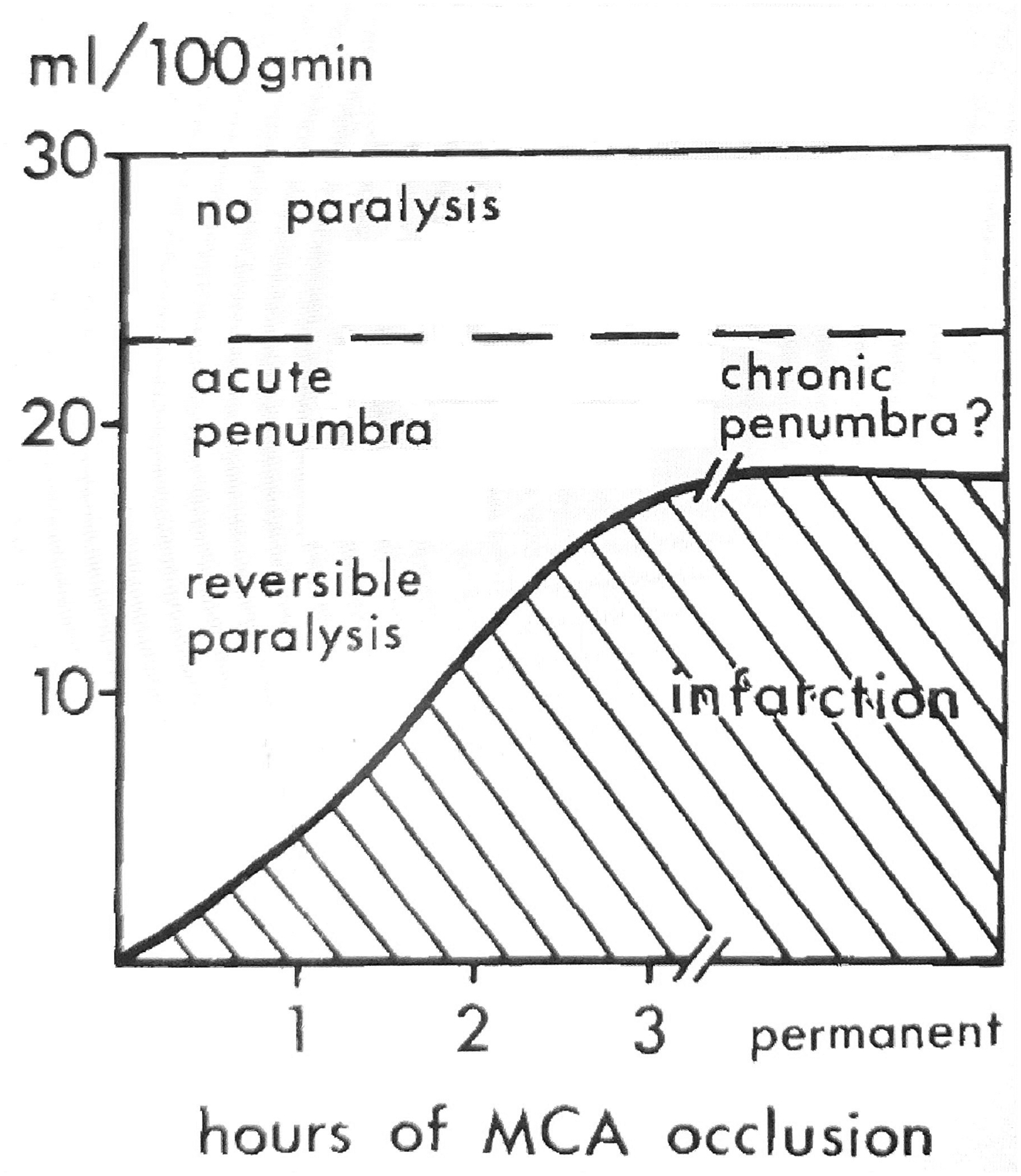
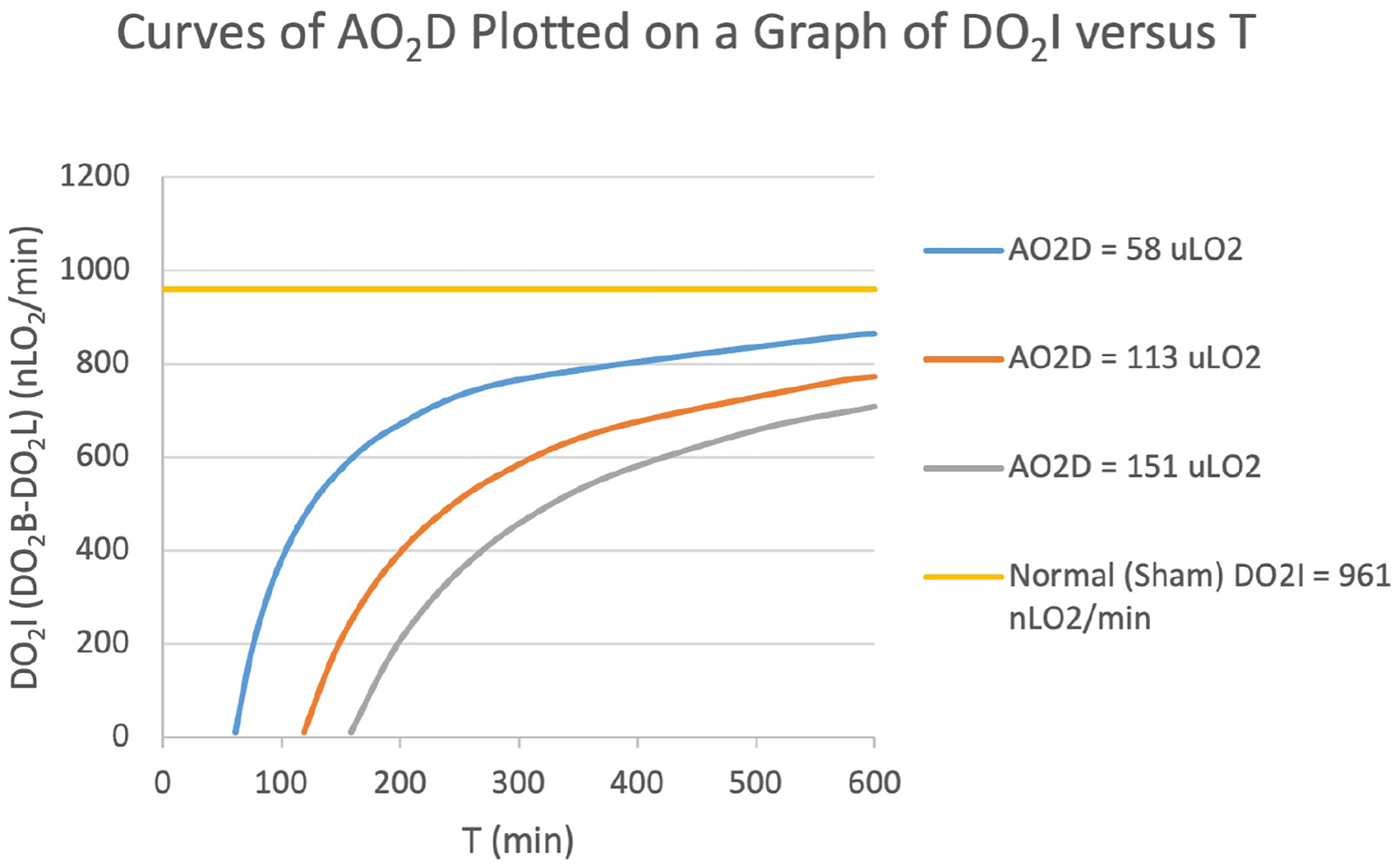
We here attempt to improve quantification of the ischemic retinal insult, that is, what is imposed on the retinal tissue by ischemia, especially in experimental models of ischemia. The ischemic retinal insult initiates the ischemic retinal injury (or outcome). Accordingly, it is reasonable to assume that the better the quantification of the insult, the better the correlation with, and thereby estimation of, the injury. The insult seldom has been quantified in terms of the relevant physiological factors, especially in connection with the rate of oxygen delivery (DO2). We here propose the accumulated oxygen deficit (AO2D) as an indicator of the ischemic retinal insult. We hypothesized that AO2D is correlated with the rate of oxygen metabolism measured 1 h after reperfusion following an episode of ischemia (MO2_1_Hr). Previously, we showed that MO2_1_Hr is related to the electroretinogram amplitude and the retinal thickness when they are measured seven days after reperfusion. We studied 27 rats, as well as 26 rats from our published data on retinal ischemia in which we had measurements of DO2 and duration of ischemia (T) of various levels and durations. We also measured DO2 in 29 rats treated with sham surgery. Ischemia was induced by either ipsilateral or bilateral common carotid artery occlusion or by ophthalmic artery occlusion, which gave a wide range of DO2. DO2 and MO2_1_Hr were evaluated based on three types of images: 1) red-free images to measure vessel diameters, 2) fluorescence images to estimate blood velocities by the displacement of intravascular fluorescent microspheres over time, and 3) phosphorescence images to quantify vascular oxygen tension from the phosphorescence lifetime of an intravascular oxygen sensitive phosphor. Loss of oxygen delivery (DO2L) was calculated as the difference between DO2 under normal/sham condition and DO2 during ischemia. AO2D, a volume of oxygen, was calculated as the product DO2L and T. Including all data, the linear relationship between AO2D and MO2_1_Hr was significant (R2 = 0.261, P = 0.0003). Limiting data to that in which T or DO2L was maximal also yielded significant relationships, and revealed that DO2L at a long duration of ischemia contributed disproportionately more than T to MO2_1_Hr. We discuss the potential of AO2D for quantifying the ischemic retinal insult, predicting the ischemic retinal injury and evaluating the likelihood of infarction.
Keywords: Imaging; Retinal blood flow; Retinal ischemia; Retinal oxygen delivery; Retinal oxygen metabolism.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest M. Shahidi holds a patent for the oxygen imaging technology. The other authors have no interests to declare.
Figures
References
-
- Alder VA, Ben-Nun J, Cringle SJ, 1990. PO2 profiles and oxygen consumption in cat retina with an occluded retinal circulation. Investigative ophthalmology & visual science 31, 1029–1034. - PubMed
-
- Ames A 3rd, 2000. CNS energy metabolism as related to function. Brain Res Brain Res Rev 34, 42–68. - PubMed
-
- Ames A 3rd, Maynard KI, Kaplan S, 1995. Protection against CNS ischemia by temporary interruption of function-related processes of neurons. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism 15, 433–439. - PubMed
-
- Auer RN, 1998. Histopathology of Cerebral Ischemia, in: Ginsberg MD, Bogousslavsky J (Ed.), Cerebrovascular Disease:Pathophysiology, Diagnosis, Management. Blackwell Science, Malden, MA, pp. 90–101.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
