

An integrative survival analysis and a systematic review of the cerebellopontine angle glioblastomas
- PMID: 36932101
- PMCID: PMC10023706
- DOI: 10.1038/s41598-023-30677-x
An integrative survival analysis and a systematic review of the cerebellopontine angle glioblastomas
Abstract
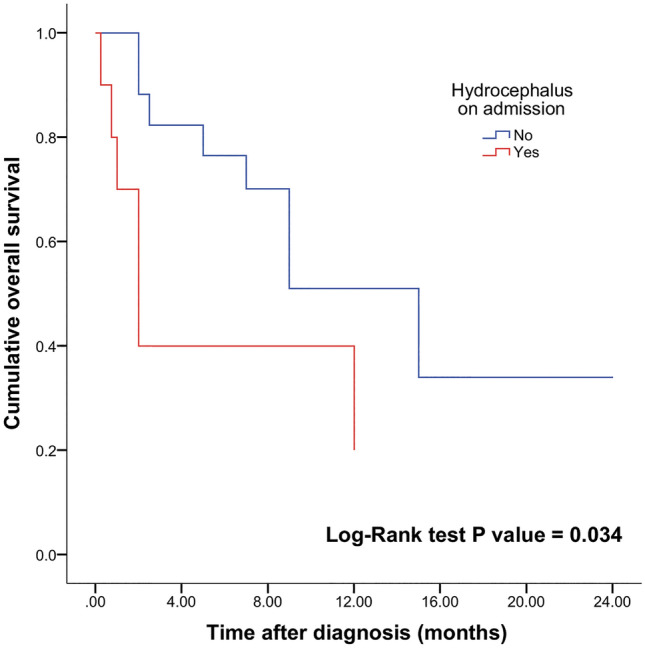
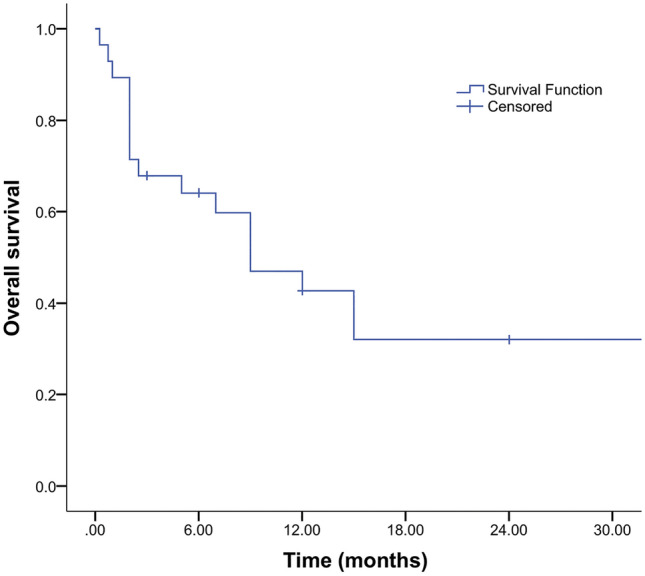
Glioblastomas presenting topographically at the cerebellopontine angle (CPA) are exceedingly rare. Given the specific anatomical considerations and their rarity, overall survival (OS) and management are not discussed in detail. The authors performed an integrative survival analysis of CPA glioblastomas. A literature search of PubMed, Scopus, and Web of Science databases was performed per PRISMA guidelines. Patient data including demographics, clinical features, neuroimaging, management, follow-up, and OS were extracted. The mean age was 39 ± 26.2 years. The mean OS was 8.9 months. Kaplan-Meier log-rank test and univariate Cox proportional-hazards model identified hydrocephalus (log-rank, p = 0.034; HR 0.34; 95% CI 0.12-0.94; p = 0.038), chemotherapy (log-rank, p < 0.005; HR 5.66; 95% CI 1.53-20.88; p = 0.009), and radiotherapy (log-rank, p < 0.0001; HR 12.01; 95% CI 3.44-41.89; p < 0.001) as factors influencing OS. Hydrocephalus (HR 3.57; 95% CI 1.07-11.1; p = 0.038) and no adjuvant radiotherapy (HR 0.12; 95% CI 0.02-0.59; p < 0.01) remained prognostic on multivariable analysis with fourfold and twofold higher risk for the time-related onset of death, respectively. This should be considered when assessing the risk-to-benefit ratio for patients undergoing surgery for CPA glioblastoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
