

Pulmonary vessel volume in idiopathic pulmonary fibrosis compared with healthy controls aged > 50 years
- PMID: 36932117
- PMCID: PMC10023743
- DOI: 10.1038/s41598-023-31470-6
Pulmonary vessel volume in idiopathic pulmonary fibrosis compared with healthy controls aged > 50 years
Abstract
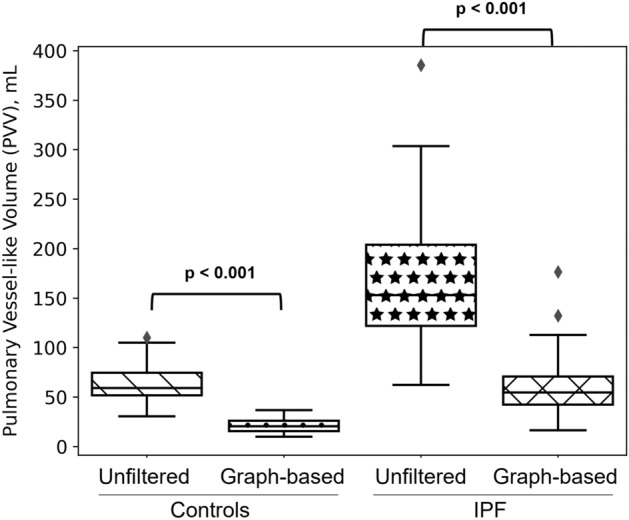
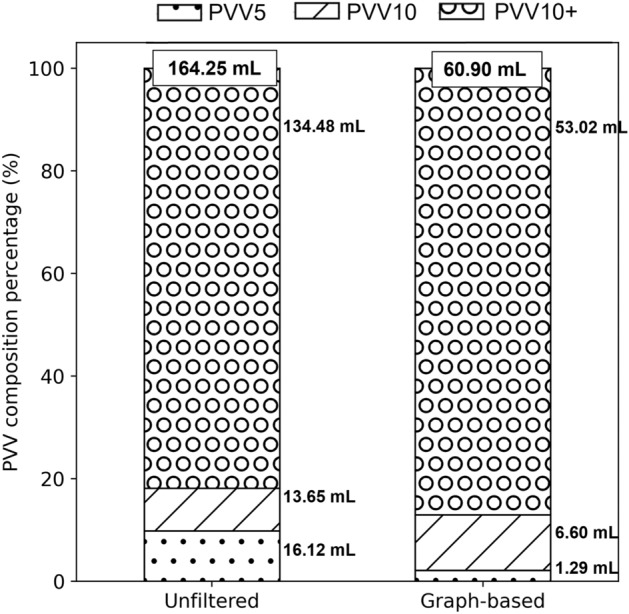
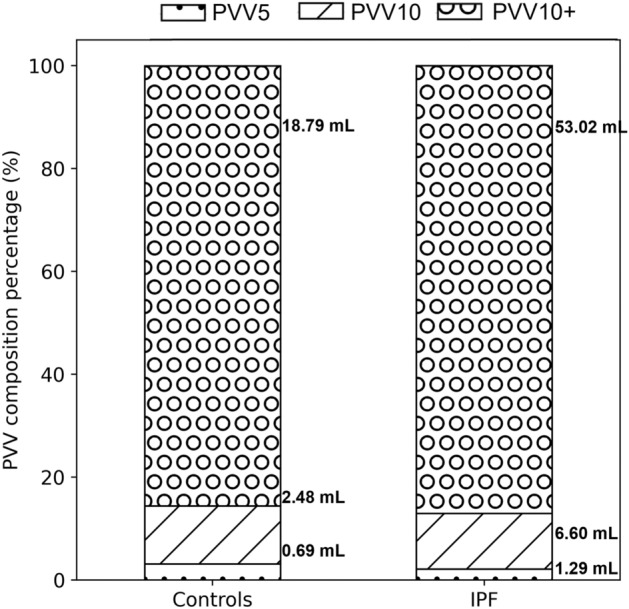
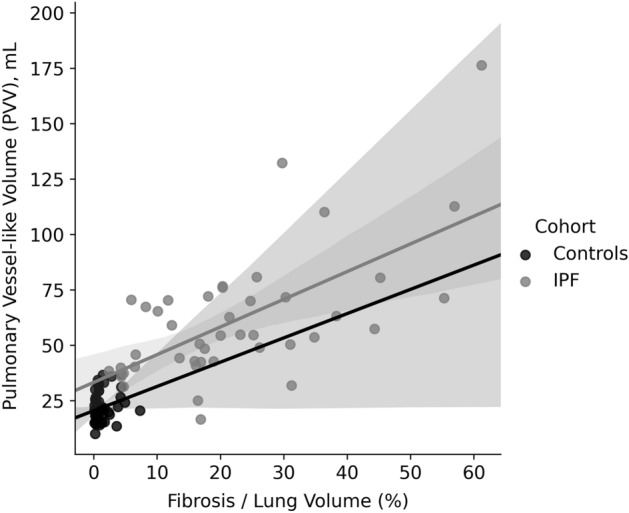
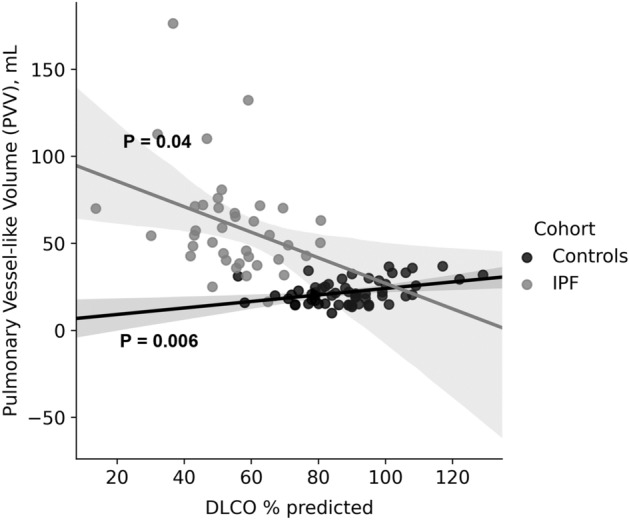
Idiopathic pulmonary fibrosis (IPF) is characterised by progressive fibrosing interstitial pneumonia with an associated irreversible decline in lung function and quality of life. IPF prevalence increases with age, appearing most frequently in patients aged > 50 years. Pulmonary vessel-like volume (PVV) has been found to be an independent predictor of mortality in IPF and other interstitial lung diseases, however its estimation can be impacted by artefacts associated with image segmentation methods and can be confounded by adjacent fibrosis. This study compares PVV in IPF patients (N = 21) with PVV from a healthy cohort aged > 50 years (N = 59). The analysis includes a connected graph-based approach that aims to minimise artefacts contributing to calculation of PVV. We show that despite a relatively low extent of fibrosis in the IPF cohort (20% of the lung volume), PVV is 2-3 times higher than in controls. This suggests that a standardised method to calculate PVV that accounts for tree connectivity could provide a promising tool to provide early diagnostic or prognostic information in IPF patients and other interstitial lung disease.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Jacob, J. et al. Mortality prediction in idiopathic pulmonary fibrosis: evaluation of computer-based CT analysis with conventional severity measures. Eur. Respir. J.49 (2017). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
