

The impact of inotersen on Neuropathy Impairment Score in patients with hereditary transthyretin amyloidosis with polyneuropathy
- PMID: 36932361
- PMCID: PMC10022100
- DOI: 10.1186/s12883-023-03116-7
The impact of inotersen on Neuropathy Impairment Score in patients with hereditary transthyretin amyloidosis with polyneuropathy
Abstract
Background: Patients with hereditary transthyretin amyloidosis (ATTRv) frequently experience symptoms of polyneuropathy (PN) that worsen over time and impair daily functioning. Previous analyses supported efficacy of inotersen, an antisense oligonucleotide, to slow neuropathic progression in patients with ATTRv-PN, as indicated by larger mean changes, relative to placebo, in total score and several subscales of the Neuropathy Impairment Score (NIS), and for the subset of NIS items specific to lower limbs (NIS-LL) for the overall study sample. A key objective of the current study was to evaluate efficacy of inotersen for slowing neuropathic progression in NIS/NIS-LL within key clinical subgroups of patients with ATTRv-PN. Additionally, for this study, responder definition (RD) thresholds were estimated for NIS/NIS-LL total and subscale scores, for the purpose of evaluating clinically meaningful benefit of inotersen at the individual patient-level.
Methods: Post hoc analyses used data from the NEURO-TTR phase 3 trial of inotersen in patients with ATTRv-PN (NCT01737398). Treatment differences in mean changes on NIS/NIS-LL total and subscale scores from baseline to week 65 were examined within patient subgroups defined by clinical characteristics. Anchor- and distribution-based approaches estimated RDs for NIS/NIS-LL scores, with responders defined as patients who did not experience clinically meaningful neuropathic progression. Responder analyses compared the proportion of patients classified as responders for each NIS/NIS-LL score between treatment arms.
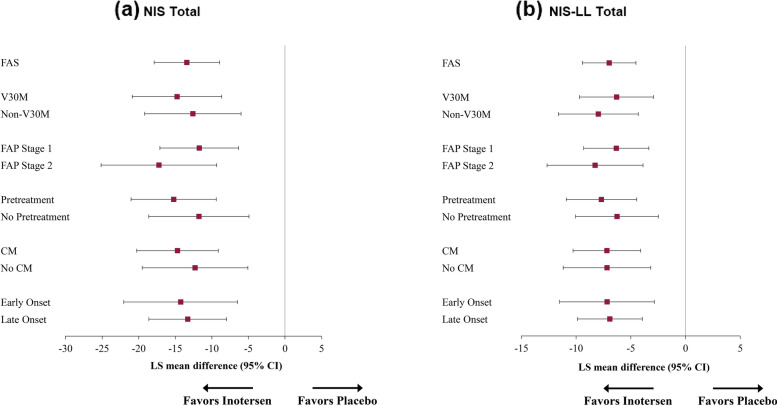
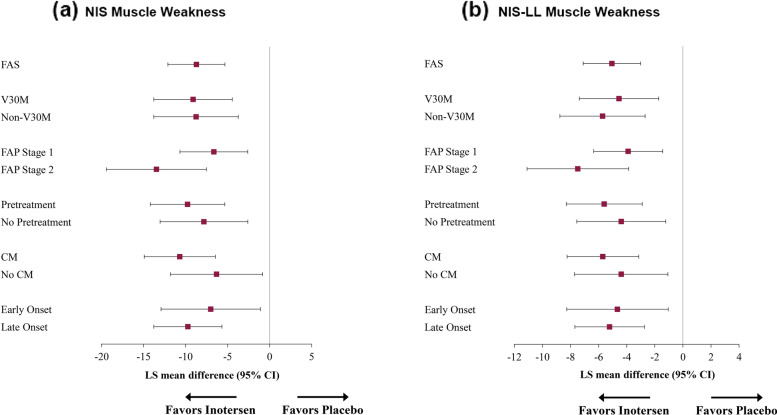
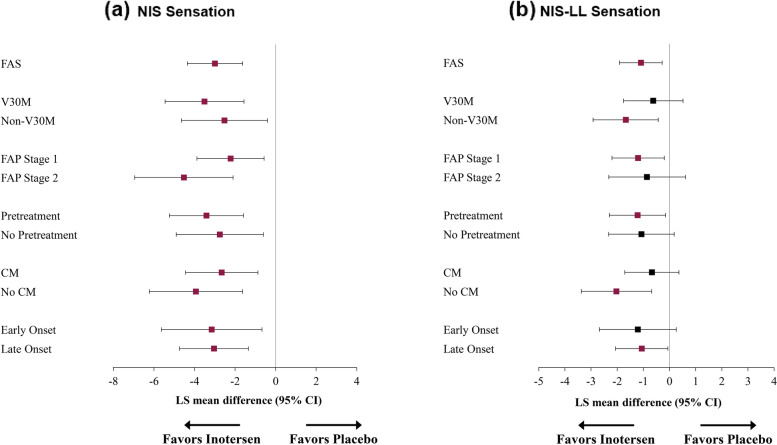
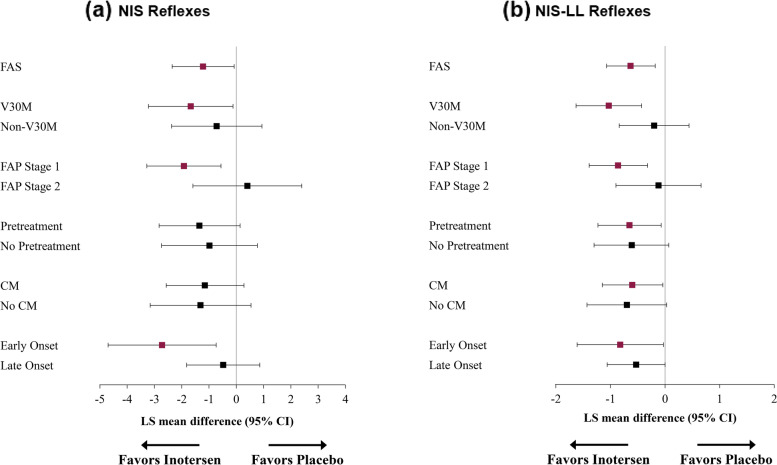
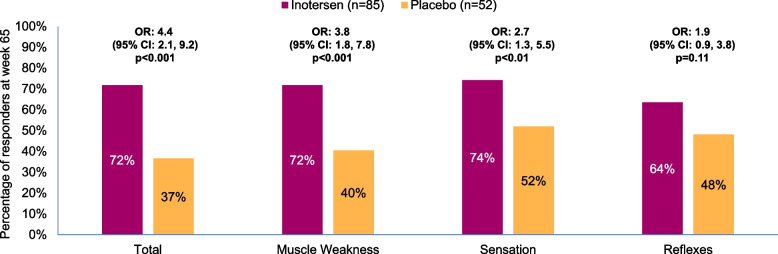
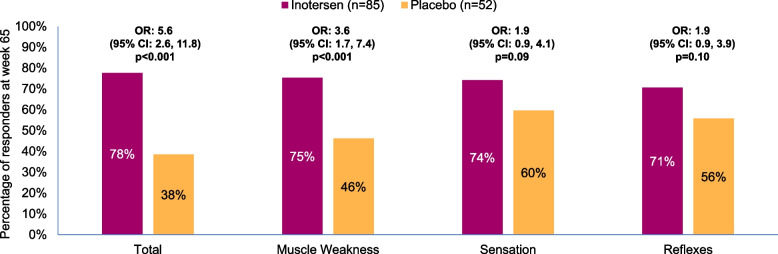
Results: Within each patient subgroup, mean increases in NIS/NIS-LL total and muscle weakness subscales were significantly smaller after 65 weeks of treatment with inotersen compared to placebo. Similar patterns were observed for some, but not all, subgroups on NIS/NIS-LL reflex subscale scores. Recommended RDs were 8.1 points for NIS total and 4.7 points for NIS-LL total. Patients receiving inotersen for 65 weeks were significantly less likely than those receiving placebo to exhibit clinically meaningful increases on NIS/NIS-LL total, muscle weakness, and sensation subscales.
Conclusions: This study supports previous evidence for efficacy of inotersen in this patient population and provides interpretation guidelines for clinically meaningful changes in NIS/NIS-LL scores.
Keywords: Hereditary transthyretin amyloidosis; Inotersen; Neuropathic progression; Neuropathy.
© 2023. The Author(s).
Conflict of interest statement
At the time of this research, AY was an employee of QualityMetric, which received payment from Ionis Pharmaceuticals Inc., to conduct these analyses and develop this manuscript; AY is currently an employee of and owns stock in Ionis Pharmaceuticals Inc. AL is an employee of QualityMetric. DB and MVL are employees of and own stock in Ionis Pharmaceuticals Inc. SK has received consulting honoraria from Ionis Pharmaceuticals, Akcea Therapeutics, Alnylam, Pfizer, and Eidos. CK has received consulting honoraria from Ionis Pharmaceuticals, Akcea Therapeutics, Argenx, CSL Behring, Alnylam, Biogen, and Sanofi.
Figures
Similar articles
-
Responder analysis for neuropathic impairment and quality-of-life assessment in patients with hereditary transthyretin amyloidosis with polyneuropathy in the NEURO-TTR study.J Neurol. 2022 Jan;269(1):323-335. doi: 10.1007/s00415-021-10635-1. Epub 2021 Jun 14. J Neurol. 2022. PMID: 34125267 Free PMC article.
-
Early Data on Long-term Impact of Inotersen on Quality-of-Life in Patients with Hereditary Transthyretin Amyloidosis Polyneuropathy: Open-Label Extension of NEURO-TTR.Neurol Ther. 2021 Dec;10(2):865-886. doi: 10.1007/s40120-021-00268-x. Epub 2021 Aug 5. Neurol Ther. 2021. PMID: 34355354 Free PMC article.
-
Rate of neuropathic progression in hereditary transthyretin amyloidosis with polyneuropathy and other peripheral neuropathies: a systematic review and meta-analysis.BMC Neurol. 2021 Feb 12;21(1):70. doi: 10.1186/s12883-021-02094-y. BMC Neurol. 2021. PMID: 33579211 Free PMC article.
-
Factors associated with increased health-related quality-of-life benefits in hereditary transthyretin amyloidosis polyneuropathy patients treated with inotersen.Muscle Nerve. 2022 Sep;66(3):319-328. doi: 10.1002/mus.27668. Epub 2022 Jul 15. Muscle Nerve. 2022. PMID: 35766224 Clinical Trial.
-
Inotersen for the treatment of adults with polyneuropathy caused by hereditary transthyretin-mediated amyloidosis.Expert Rev Clin Pharmacol. 2019 Aug;12(8):701-711. doi: 10.1080/17512433.2019.1635008. Epub 2019 Jul 3. Expert Rev Clin Pharmacol. 2019. PMID: 31268366 Review.
Cited by
-
Clinical differential factors in patients with hereditary transthyretin amyloidosis with Val142Ile and Ser43Asn mutations.Orphanet J Rare Dis. 2024 Dec 20;19(1):474. doi: 10.1186/s13023-024-03496-0. Orphanet J Rare Dis. 2024. PMID: 39707389 Free PMC article.
-
Etiological Treatment of Cardiac Amyloidosis: Standard of Care and Future Directions.Curr Heart Fail Rep. 2025 Apr 15;22(1):16. doi: 10.1007/s11897-025-00701-4. Curr Heart Fail Rep. 2025. PMID: 40232627 Free PMC article. Review.
-
Estimating Meaningful Differences in Measures of Neuropathic Impairment, Health-Related Quality of Life, and Nutritional Status in Patients With Hereditary Transthyretin Amyloidosis.Muscle Nerve. 2025 Jan;71(1):96-107. doi: 10.1002/mus.28299. Epub 2024 Nov 17. Muscle Nerve. 2025. PMID: 39552102 Free PMC article. Clinical Trial.
-
Short-term treatment of CIDP with efgartigimod: a case series in China.Front Immunol. 2025 May 1;16:1533167. doi: 10.3389/fimmu.2025.1533167. eCollection 2025. Front Immunol. 2025. PMID: 40375986 Free PMC article.
-
The Coming Age of Antisense Oligos for the Treatment of Hepatic Ischemia/Reperfusion (IRI) and Other Liver Disorders: Role of Oxidative Stress and Potential Antioxidant Effect.Antioxidants (Basel). 2024 May 31;13(6):678. doi: 10.3390/antiox13060678. Antioxidants (Basel). 2024. PMID: 38929116 Free PMC article. Review.
References
-
- Lin X, Yarlas A, Vera-Llonch M, Baranwal N, Biber J, Brown D, et al. Rate of neuropathic progression in hereditary transthyretin amyloidosis with polyneuropathy and other peripheral neuropathies: a systematic review and meta-analysis. BMC Neurol. 2021;21(1):70. doi: 10.1186/s12883-021-02094-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
