

Yoga and massage are associated with small experimental placebo effects in chronic orofacial pain
- PMID: 36932918
- PMCID: PMC11001249
- DOI: 10.1002/ejp.2111
Yoga and massage are associated with small experimental placebo effects in chronic orofacial pain
Abstract
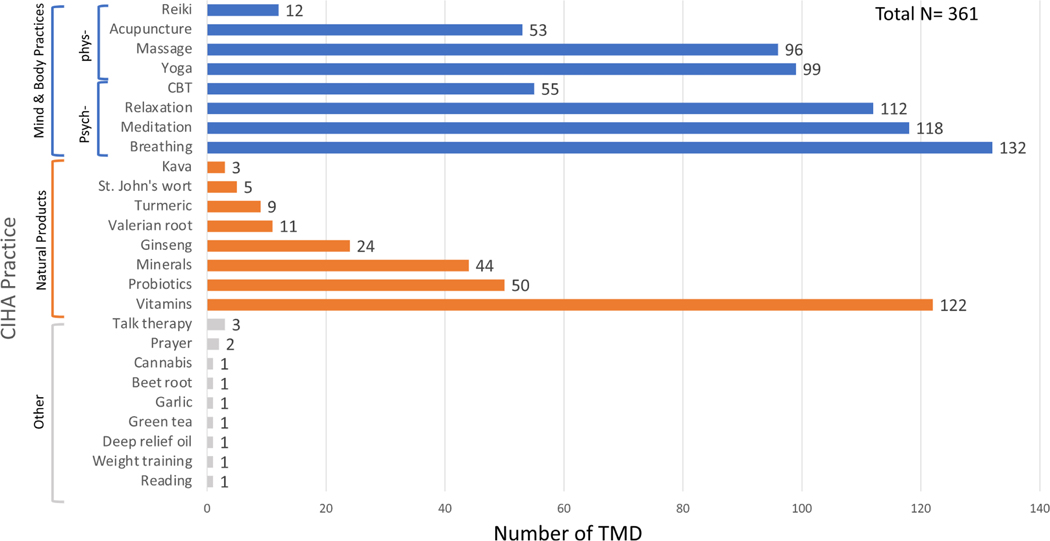
Background: Complementary and Integrative Health Approaches (CIHA), including but not limited to, natural products and Mind and Body Practices (MBPs), are promising non-pharmacological adjuvants to the arsenal of pain management therapeutics. We aim to establish possible relationships between use of CIHA and the capacity of descending pain modulatory system in the form of occurrence and magnitude of placebo effects in a laboratory setting.
Methods: This cross-sectional study investigated the relationship between self-reported use of CIHA, pain disability, and experimentally induced placebo hypoalgesia in chronic pain participants suffering from Temporomandibular Disorders (TMD). In the 361 enrolled TMD participants, placebo hypoalgesia was measured using a well-established paradigm with verbal suggestions and conditioning cues paired with distinct heat painful stimulations. Pain disability was measured with the Graded Chronic Pain Scale, and use of CIHA were recorded with a checklist as part of the medical history.
Results: Use of physically oriented MBPs (e.g., yoga and massage) was associated with reduced placebo effects (F1,2110.44 = 23.15, p < 0.001, Cohen's d = 0.171). Further, linear regressions indicated that greater number of physically oriented MBPs predicted smaller placebo effects (β = -0.17, p = 0.002), and less likelihood of being a placebo responder (OR = 0.70, p = 0.004). Use of psychologically oriented MBPs and natural product were not associated with placebo effects magnitude and responsiveness.
Conclusions: Our findings suggest that use of physically oriented CIHA was associated with experimental placebo effects possibly through an optimized capability to recognize distinct somatosensorial stimulations. Future research is needed to understand the mechanisms underlying placebo-induced pain modulation in CIHA users.
Significance: Chronic pain participants who use physically oriented mind-body practices, such as yoga and massage, demonstrated attenuated experimentally induced placebo hypoalgesia in comparison with those who do not use them. This finding disentangled the relationship between use of complementary and integrative approaches and placebo effects, providing the potential therapeutic perspective of endogenous pain modulation in chronic pain management.
© 2023 European Pain Federation - EFIC ®.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest to declare.
Figures



References
-
- Allan LG, & Siegel S. (2002). A signal detection theory analysis of the placebo effect. Evaluation & the Health Professions, 25, 410–420. - PubMed
-
- Arandia IR, & Di Paolo EA (2022). On symptom perception, placebo effects, and the Bayesian brain. Pain, 163, e604. - PubMed
-
- Arienti C. (2021). Can herbal medicinal products or preparations alleviate neuropathic pain in adults? A Cochrane review summary with commentary. NeuroRehabilitation, 48, 149–152. - PubMed
-
- Astin JA (1998). Why patients use alternative medicine: Results of a national study. JAMA, 279,1548–1553. - PubMed
-
- Astin JA (2004). Mind-body therapies for the management of pain. The Clinical Journal of Pain, 20, 27–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
