

Prediction of morbidity and mortality after early cholecystectomy for acute calculous cholecystitis: results of the S.P.Ri.M.A.C.C. study
- PMID: 36934276
- PMCID: PMC10024826
- DOI: 10.1186/s13017-023-00488-6
Prediction of morbidity and mortality after early cholecystectomy for acute calculous cholecystitis: results of the S.P.Ri.M.A.C.C. study
Abstract
Background: Less invasive alternatives than early cholecystectomy (EC) for acute calculous cholecystitis (ACC) treatment have been spreading in recent years. We still lack a reliable tool to select high-risk patients who could benefit from these alternatives. Our study aimed to prospectively validate the Chole-risk score in predicting postoperative complications in patients undergoing EC for ACC compared with other preoperative risk prediction models.
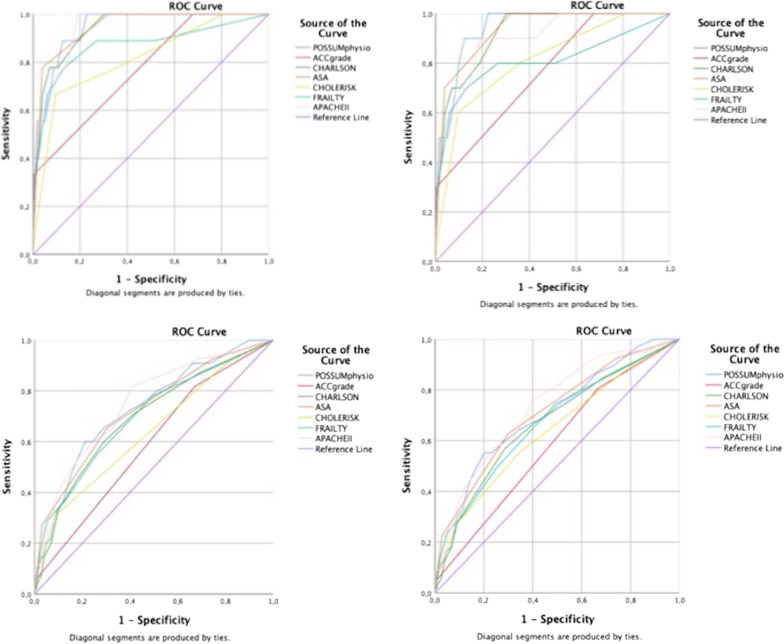
Method: The S.P.Ri.M.A.C.C. study is a World Society of Emergency Surgery prospective multicenter observational study. From 1st September 2021 to 1st September 2022, 1253 consecutive patients admitted in 79 centers were included. The inclusion criteria were a diagnosis of ACC and to be a candidate for EC. A Cochran-Armitage test of the trend was run to determine whether a linear correlation existed between the Chole-risk score and a complicated postoperative course. To assess the accuracy of the analyzed prediction models-POSSUM Physiological Score (PS), modified Frailty Index, Charlson Comorbidity Index, American Society of Anesthesiologist score (ASA), APACHE II score, and ACC severity grade-receiver operating characteristic (ROC) curves were generated. The area under the ROC curve (AUC) was used to compare the diagnostic abilities.
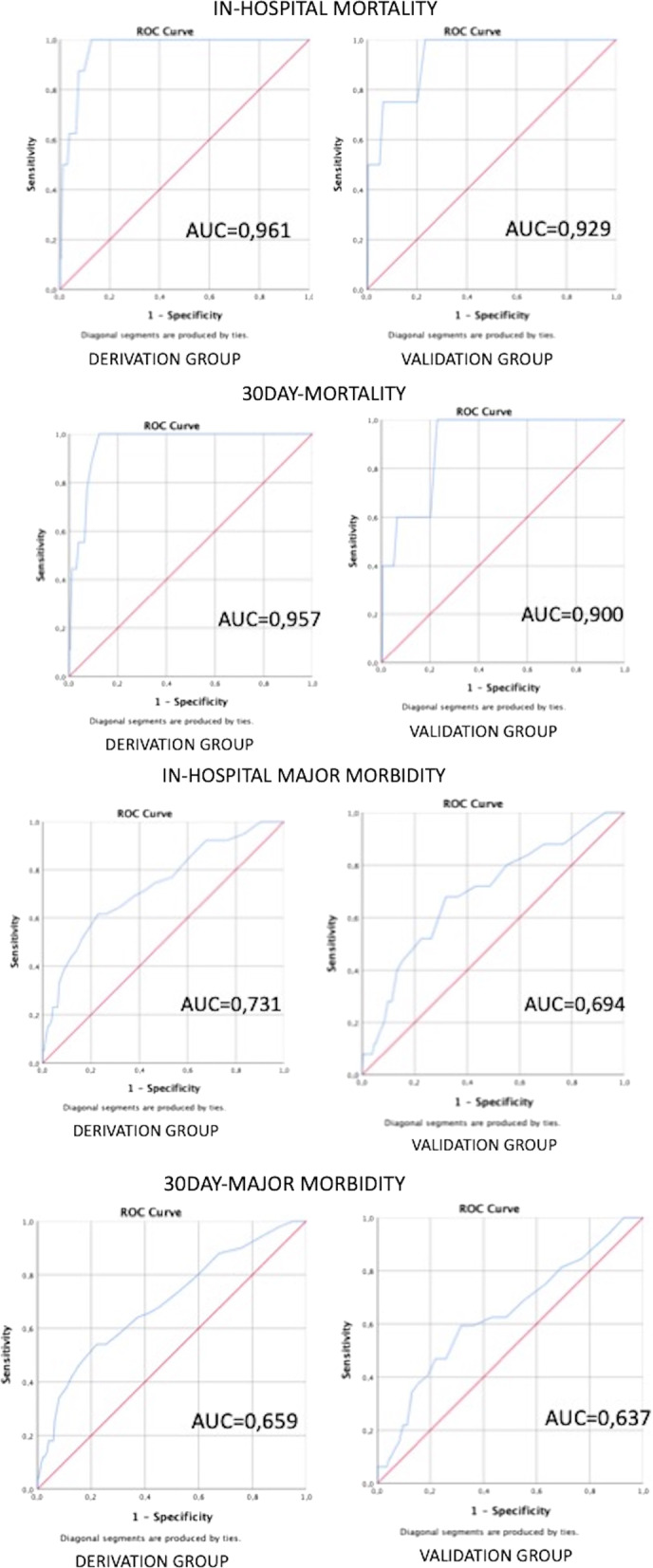
Results: A 30-day major morbidity of 6.6% and 30-day mortality of 1.1% were found. Chole-risk was validated, but POSSUM PS was the best risk prediction model for a complicated course after EC for ACC (in-hospital mortality: AUC 0.94, p < 0.001; 30-day mortality: AUC 0.94, p < 0.001; in-hospital major morbidity: AUC 0.73, p < 0.001; 30-day major morbidity: AUC 0.70, p < 0.001). POSSUM PS with a cutoff of 25 (defined in our study as a 'Chole-POSSUM' score) was then validated in a separate cohort of patients. It showed a 100% sensitivity and a 100% negative predictive value for mortality and a 96-97% negative predictive value for major complications.
Conclusions: The Chole-risk score was externally validated, but the CHOLE-POSSUM stands as a more accurate prediction model. CHOLE-POSSUM is a reliable tool to stratify patients with ACC into a low-risk group that may represent a safe EC candidate, and a high-risk group, where new minimally invasive endoscopic techniques may find the most useful field of action.
Trial registration: ClinicalTrial.gov NCT04995380.
Keywords: Acute cholecystitis; Cholecystectomy; POSSUM; Surgical risk.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
