

Heart failure with reduced ejection fraction and atrial fibrillation: a Sub-Saharan African perspective
- PMID: 36934444
- PMCID: PMC10192282
- DOI: 10.1002/ehf2.14332
Heart failure with reduced ejection fraction and atrial fibrillation: a Sub-Saharan African perspective
Abstract
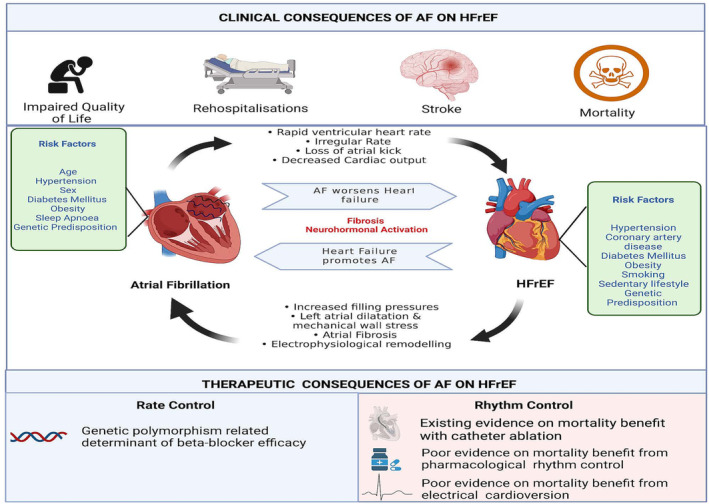
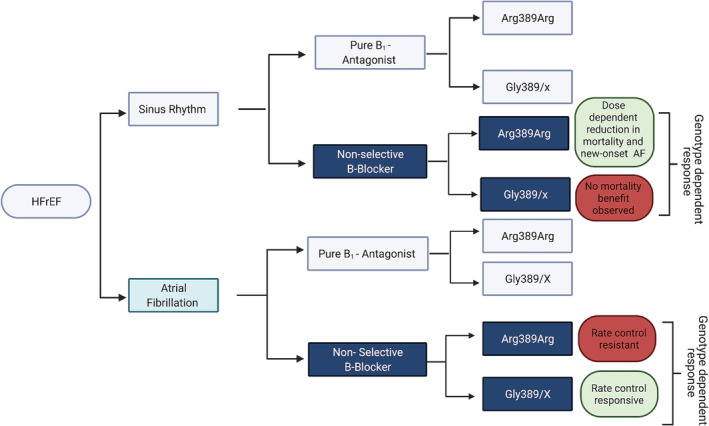
Cardiovascular diseases are a well-established cause of death in high-income countries. In the last 20 years, Sub-Saharan Africa (SSA) has seen one of the sharpest increases in cardiovascular disease-related mortality, superseding that of infectious diseases, including HIV/AIDS, in South Africa. This increase is evidenced by a growing burden of heart failure and atrial fibrillation (AF) risk factors. AF is a common comorbidity of heart failure with reduced ejection fraction (HFrEF), which predisposes to an increased risk of stroke, rehospitalizations, and mortality compared with patients in sinus rhythm. AF had the largest relative increase in cardiovascular disease burden between 1990 and 2010 in SSA and the second highest (106.4%) increase in disability-adjusted life-years (DALY) between 1990 and 2017. Over the last decade, significant advancements in the management of both HFrEF and AF have emerged. However, managing HFrEF/AF remains a clinical challenge for physicians, compounded by the suboptimal efficacy of guideline-mandated pharmacotherapy in this group of patients. There may be an essential role for racial differences and genetic influence on therapeutic outcomes of HFrEF/AF patients, further complicating our overall understanding of the disease and its pathophysiology. In SSA, the lack of accurate and up-to-date epidemiological data on this subgroup of patients presents a challenge in our quest to prevent and reduce adverse outcomes. This narrative review provides a contemporary overview of the epidemiology of HFrEF/AF in SSA. We highlight important differences in the demographic and aetiological profile and the management of this subpopulation, emphasizing what is currently known and, more importantly, what is still unknown about HFrEF/AF in SSA.
Keywords: Atrial fibrillation; Heart failure with reduced ejection fraction (HFrEF); Sub-Saharan Africa.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, Dzudie A, Kouam CK, Suliman A, Schrueder N, Yonga G, Ba SA, Maru F, Alemayehu B, Edwards C, Davison BA, Cotter G, Sliwa K. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries. Arch Intern Med. 2012; 172: 1386–1394. - PubMed
-
- Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: epidemiological profile and challenges. Nat Rev Cardiol. 2017; 14: 273–293. - PubMed
-
- Stewart S, Wilkinson D, Hansen C, Vaghela V, Mvungi R, McMurray J, Sliwa K. Predominance of heart failure in the Heart of Soweto Study cohort. Circulation. 2008; 118: 2360–2367. - PubMed
-
- Ajayi AA, Sofowora GG, Ladipo GO. Explaining heart failure hyper‐mortality in Sub Saharan Africa: global genomic and environmental contribution review. J Natl Med Assoc. 2020; 112: 141–157. - PubMed
-
- Sliwa K, Mayosi BM. Recent advances in the epidemiology, pathogenesis and prognosis of acute heart failure and cardiomyopathy in Africa. Heart. 2013; 99: 1317–1322. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials