

Single priming and booster dose of ten-valent and 13-valent pneumococcal conjugate vaccines and Streptococcus pneumoniae colonisation in children in South Africa: a single-centre, open-label, randomised trial
- PMID: 36934731
- PMCID: PMC10127219
- DOI: 10.1016/S2352-4642(23)00025-1
Single priming and booster dose of ten-valent and 13-valent pneumococcal conjugate vaccines and Streptococcus pneumoniae colonisation in children in South Africa: a single-centre, open-label, randomised trial
Abstract
Background: Pneumococcal conjugate vaccine (PCV) immunisation has reduced vaccine-serotype colonisation and invasive pneumococcal disease in South Africa, providing the opportunity to consider transitioning from a two-dose (2 + 1) to one-dose (1 + 1) primary series and a booster dose.
Methods: In this single-centre, open-label, randomised trial done in South Africa, infants aged 35-49 days without HIV infection, without childhood immunisations except for BCG and polio, and with gestation age at delivery of at least 37 weeks of age, a birthweight of at least 2500 g, and weight of at least 3500 g at the time of enrolment were randomly assigned (1:1:1:1:1:1), through block randomisation (block size of 30), to receive a single priming dose of ten-valent PCV (PCV10) or 13-valent PCV (PCV13) at either 6 weeks (6-week 1 + 1 group) or 14 weeks (14-week 1 + 1 group), compared with two priming doses at 6 weeks and 14 weeks (2 + 1 group), followed by a booster dose at 9 months of age in all groups. The primary objective of the trial has been published previously. We report the secondary objective of the effect of alternative doses of PCV10 and PCV13 on serotype-specific Streptococcus pneumoniae colonisation at 9 months, 15 months, and 18 months of age and a further exploratory analysis in which we assessed non-inferiority of serotype-specific serum IgG geometric mean concentrations 1 month after the booster (10 months of age) and the percentage of participants with serotype-specific IgG titre above the putative thresholds associated with a risk reduction of serotype-specific colonisation between the 1 + 1 and 2 + 1 groups for both vaccines. Non-inferiority was established if the lower limit of the 95% CI for the difference between the proportion of participants (1 + 1 group vs 2 + 1 group) above the putative thresholds was greater than or equal to -10%. All analyses were done in the modified intention-to-treat population, which included all participants who received PCV10 or PCV13 according to assigned randomisation group and for whom laboratory results were available. The trial is registered with ClinicalTrials.gov, NCT02943902.
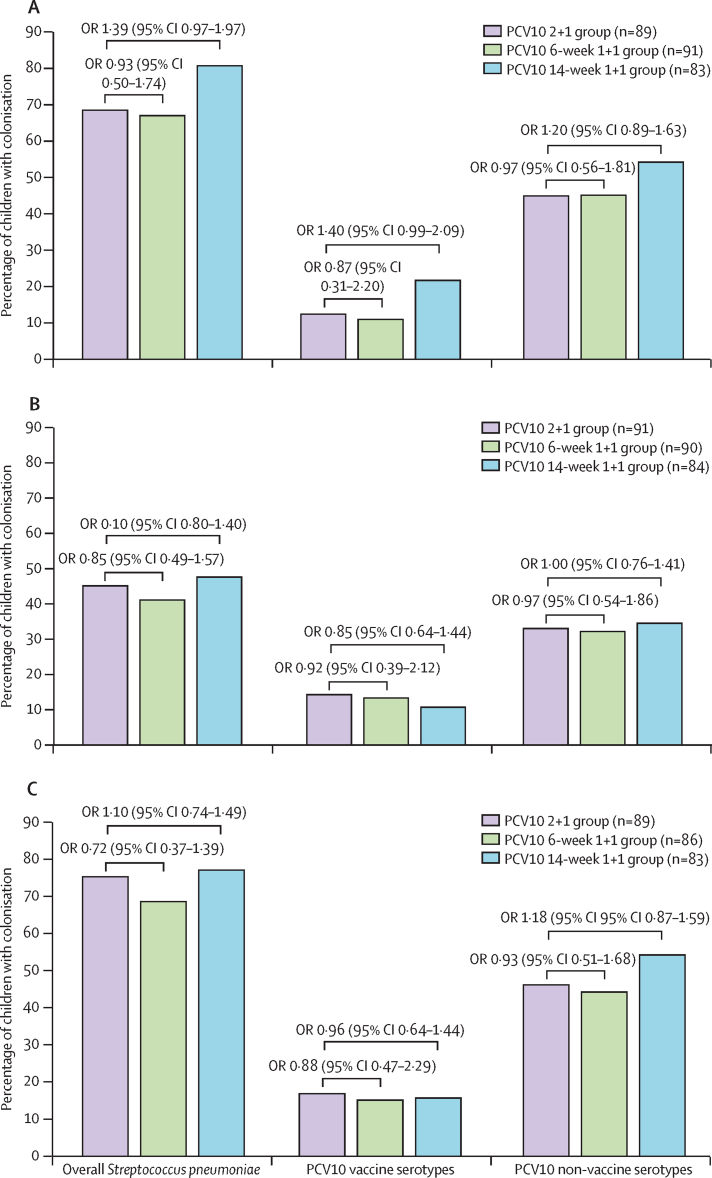
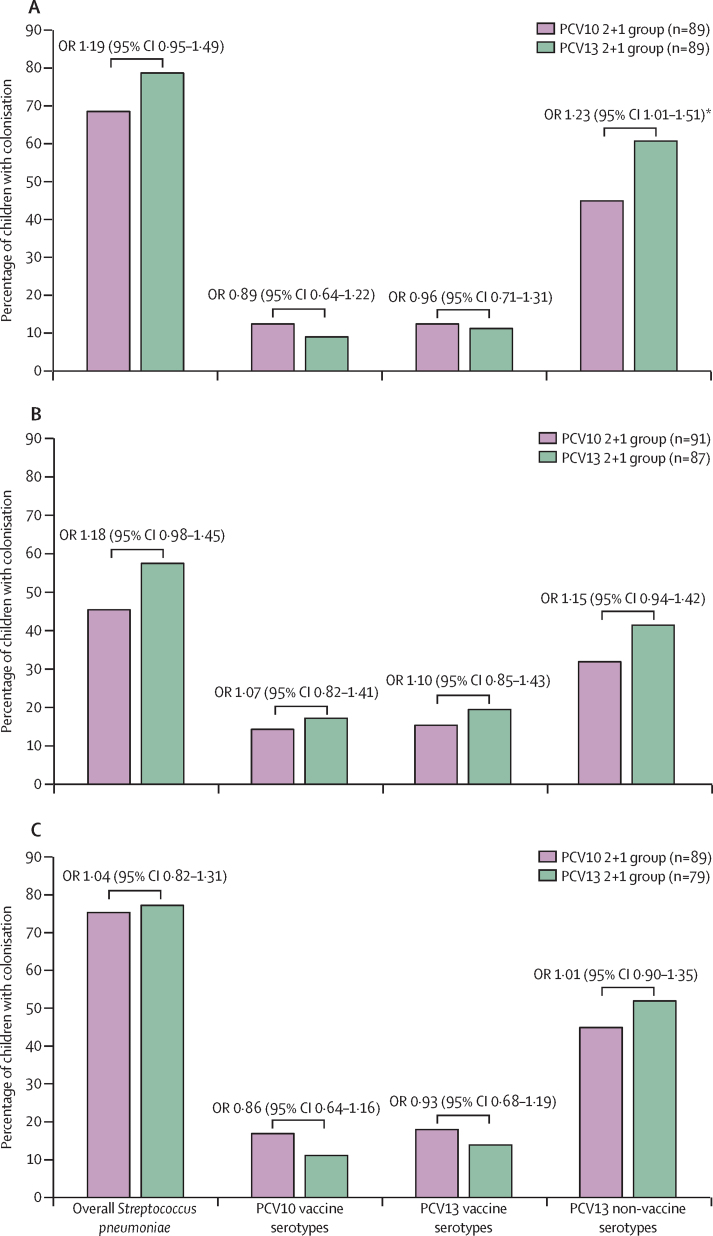
Findings: 1564 nasopharyngeal swabs were available for molecular serotyping from 600 infants who were enrolled (100 were randomly assigned to each of the six study groups) between Jan 9 and Sept 20, 2017. There was no significant difference in the prevalence of overall or non-vaccine serotype colonisation between all PCV13 or PCV10 groups. PCV13 serotype colonisation was lower at 15 months of age in the 14-week 1 + 1 group than in the 2 + 1 group (seven [8%] of 85 vs 17 [20%] of 87; odds ratio 0·61 [95% CI 0·38-0·97], p=0·037), but no difference was seen at 9 months (nine [11%] of 86 vs ten [11%] of 89; 0·92 [0·60-1·55], p=0·87) or 18 months (nine [11%] of 85 vs 11 [14%] of 87; 0·78 [0·45-1·22], p=0·61). Compared with the PCV13 2 + 1 group, both PCV13 1 + 1 groups did not meet the non-inferiority criteria for serotype-specific anti-capsular antibody concentrations above the putative thresholds purportedly associated with risk reduction for colonisation; however, the PCV10 14-week 1 + 1 group was non-inferior to the PCV10 2 + 1 group.
Interpretation: The serotype-specific colonisation data reported in this study together with the primary immunogenicity endpoints of the control trial support transitioning to a reduced 1 + 1 schedule in South Africa. Ongoing monitoring of colonisation should, however, be undertaken immediately before and after transitioning to a PCV 1 + 1 schedule to serve as an early indicator of whether PCV 1 + 1 could lead to an increase in vaccine-serotype disease.
Funding: The Bill & Melinda Gates Foundation.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests GlaxoSmithKline (GSK) awarded grant funding to Wits VIDA for research related to PCVs. Furthermore, GSK and Pfizer have funded Wits VIDA to undertake non-pneumococcal research. However, neither Pfizer nor GSK contributed to the funding of this study. JRD has received grants from the Poliomyelitis Research Foundation, consultation fees from the international AIDS Vaccine Initiative, and payment from Sanofi-Aventis South Africa and Sci Mentum for work not related to this manuscript. CPO has received grants from Pfizer and the Bill & Melinda Gates Foundation, payment from Sanofi-Aventis South Africa, and support from the Gates Foundation to attend a meeting unrelated to this work. SAM has received grants from Pfizer, Minervax, GSK, the Gates Foundation, and the South African Medical Research Council, and he has received honoraria and support to attend a meeting from GSK and MSD unrelated to this work. CLC has received grants from Sanofi and Duetsche Gesellschaft fur Internationale Zusammenarbeit. All other authors declare no competing interests.
Figures

Comment in
-
Progress towards reduced-dose pneumococcal vaccine schedules for children in Africa.Lancet Child Adolesc Health. 2023 May;7(5):299-301. doi: 10.1016/S2352-4642(23)00055-X. Epub 2023 Mar 16. Lancet Child Adolesc Health. 2023. PMID: 36934732 No abstract available.
References
-
- Madhi SA, Groome MJ, Zar HJ, et al. Effectiveness of pneumococcal conjugate vaccine against presumed bacterial pneumonia hospitalisation in HIV-uninfected South African children: a case-control study. Thorax. 2015;70:1149–1155. - PubMed
-
- Pilishvili T, Lexau C, Farley MM, et al. Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J Infect Dis. 2010;201:32–41. - PubMed
-
- von Gottberg A, de Gouveia L, Tempia S, et al. Effects of vaccination on invasive pneumococcal disease in South Africa. N Engl J Med. 2014;371:1889–1899. - PubMed
-
- Madhi SA, Cohen C, von Gottberg A. Introduction of pneumococcal conjugate vaccine into the public immunization program in South Africa: translating research into policy. Vaccine. 2012;30(suppl 3):C21–C27. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
