

Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: a randomised, placebo-controlled phase 2 trial
- PMID: 36934740
- PMCID: PMC10792518
- DOI: 10.1016/S2468-1253(23)00068-7
Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: a randomised, placebo-controlled phase 2 trial
Abstract
Background: Patients with non-alcoholic steatohepatitis (NASH)-related cirrhosis are at high risk of liver-related and all-cause morbidity and mortality. We investigated the efficacy and safety of the glucagon-like peptide-1 analogue semaglutide in patients with NASH and compensated cirrhosis.
Methods: This double-blind, placebo-controlled phase 2 trial enrolled patients from 38 centres in Europe and the USA. Adults with biopsy-confirmed NASH-related cirrhosis and body-mass index (BMI) of 27 kg/m2 or more were randomly assigned (2:1) to receive either once-weekly subcutaneous semaglutide 2·4 mg or visually matching placebo. Patients were randomly allocated via an interactive web response system, stratified by presence or absence of type 2 diabetes. Patients, investigators, and those assessing outcomes were masked to treatment assignment. The primary endpoint was the proportion of patients with an improvement in liver fibrosis of one stage or more without worsening of NASH after 48 weeks, assessed by biopsy in the intention-to-treat population. Safety was assessed in all patients who received at least one dose of study drug. The trial is closed and completed, and registered with ClinicalTrials.gov, number NCT03987451.
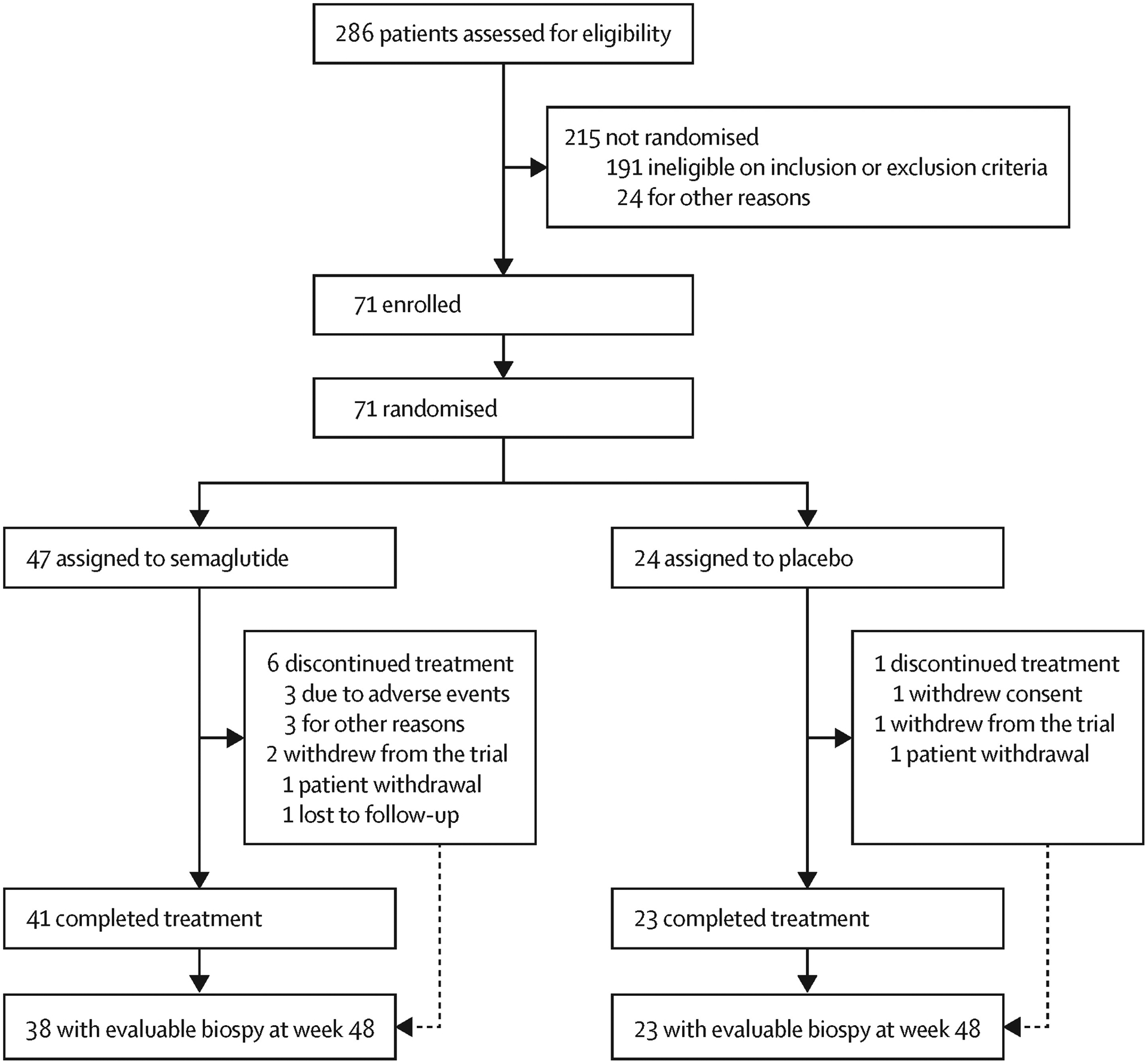
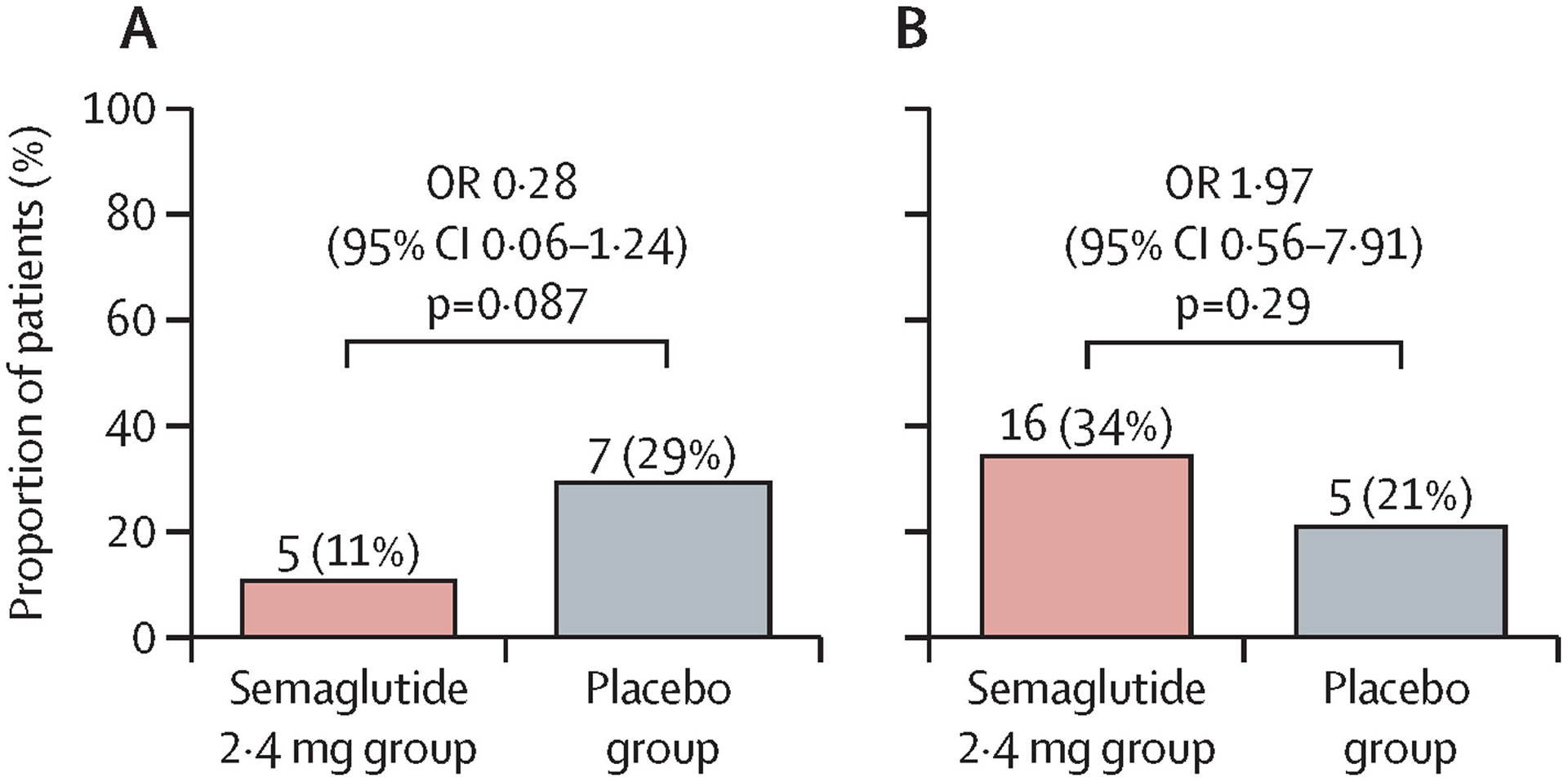
Findings: 71 patients were enrolled between June 18, 2019, and April 22, 2021; 49 (69%) patients were female and 22 (31%) were male. Patients had a mean age of 59·5 years (SD 8·0) and mean BMI of 34·9 kg/m2 (SD 5·9); 53 (75%) patients had diabetes. 47 patients were randomly assigned to the semaglutide group and 24 to the placebo group. After 48 weeks, there was no statistically significant difference between the two groups in the proportion of patients with an improvement in liver fibrosis of one stage or more without worsening of NASH (five [11%] of 47 patients in the semaglutide group vs seven [29%] of 24 in the placebo group; odds ratio 0·28 [95% CI 0·06-1·24; p=0·087). There was also no significant difference between groups in the proportion of patients who achieved NASH resolution (p=0·29). Similar proportions of patients in each group reported adverse events (42 [89%] patients in the semaglutide group vs 19 [79%] in the placebo group) and serious adverse events (six [13%] vs two [8%]). The most common adverse events were nausea (21 [45%] vs four [17%]), diarrhoea (nine [19%] vs two [8%]), and vomiting (eight [17%] vs none). Hepatic and renal function remained stable. There were no decompensating events or deaths.
Interpretation: In patients with NASH and compensated cirrhosis, semaglutide did not significantly improve fibrosis or achievement of NASH resolution versus placebo. No new safety concerns were raised.
Funding: Novo Nordisk A/S.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests RL, MFA, MJA, EL, VR, AJS, JMS, and PNN were investigators in the trial and received grants from the study sponsor paid to their institutions to conduct the study. RL is co-founder of LipoNexus Inc, and a consultant to Aardvark Therapeutics, Altimmune, Anylam/Regeneron, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Bristol Myers Squibb, CohBar, Eli Lilly, Galmed, Gilead, Glympse bio, Hightide, Inipharma, Intercept, Inventiva, Ionis, Janssen, Madrigal, Metacrine, NGM Biopharmaceuticals, Novartis, Novo Nordisk, Merck, Pfizer, Sagimet, Theratechnologies, 89bio, Terns Pharmaceuticals, and Viking Therapeutics. In addition, his institutions have received research grants from Arrowhead Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galectin Therapeutics, Galmed Pharmaceuticals, Gilead, Hanmi, Intercept, Inventiva, Ionis, Janssen, Madrigal Pharmaceuticals, Merck, NGM Biopharmaceuticals, Novo Nordisk, Pfizer, Sonic Incytes, and Terns Pharmaceuticals. MFA has received research/grant support from Allergan, Boeringher Ingelheim, BMS, Celgene, Durect, Enanta, Enyo, Galmed, Genentech, Gilead, Hanmi, Intercept, Inventiva, Madrigal, Novo Nordisk, Poxel, TARGET Pharma, and Viking; has acted as a consultant for Hanmi, NGM, BMS, 89bio, Madrigal, Intercept, Merck, Inventiva, Novo Nordisk, Sonic Incytes, and Theratechnologies; has served as a speaker for Clinical Care Options, Medscape, Fishawack LLC, and Terra Firma; has received royalties from UptoDate; and holds stock in Pfizer. MJA has received consultation fees, speaker fees, and research grants from Novo Nordisk and speaker fees and consultation fees from Norgine. JS has acted as a consultant for Apollo Endoscopy, Bristol Myers Squibb, Boehringer Ingelheim, Echosens, Genfit, Gilead Sciences, Intercept Pharmaceuticals, Madrigal, Merck, Nordic Bioscience, Novartis, Pfizer, Roche, Sanofi, and Siemens Healthcare GmbH; received research funding from Boehringer Ingelheim, Gilead Sciences, and Siemens Healthcare GmbH; and received speaker honorarium from Falk Foundation and Madrigal. MJ, MSK, and NK are employees of Novo Nordisk A/S; MSK and MJ are shareholders in Novo Nordisk A/S. EL has received research/grant support from 89bio, AbbVie, Akero Therapeutics, Allergan, Alnylam Pharmaceuticals, Amgen, Ascelia Pharma, Assemblybio, AstraZeneca, Axcella Health, Biocryst Pharmaceuticals, Bird Rock Bio, Boehringer Ingelheim, Bristol Myers Squibb, Conatus Pharmaceuticals, Cymabay Therapeutics, CytoDyn, DSM, Durect Corporation, Eli Lilly and Company, Enanta Pharmaceuticals, Enyo Pharma, Exalenz Bioscience, Galectin Therapeutics, Galmed Pharmaceuticals, Genfit, Genentech, Gilead Sciences, GlaxoSmithKline, Hanmi Pharmaceuticals, Hightide Biopharma, Intercept Pharmaceuticals, Inventiva, Janssen Pharmaceuticals, Laboratory for Advanced Medicine, Loxo Oncology, Madrigal Pharmaceuticals, Merck & Co, Metacrine, NGM Biopharmaceuticals, Northsea Therapeutics, Novartis, Novo Nordisk, Pfizer, Poxel, Roche, Sagimet Biosciences, Synlogic Therapeutics, Terns Pharmaceuticals, Viking Therapeutics, and Zydus Pharmaceuticals; has acted as a consultant for Akero, Boehringer Ingelheim, BMS, Intercept, Novo Nordisk, Metacrine, Sagimet, and Terns; and has received speaker honorarium from Gilead Sciences, AbbVie, and Intercept. AJS is President of Sanyal Biotechnology and has stock options in Exhalenz, Genfit, Hemoshear, Durect, Indalo, Northsea, Tiziana, and Rivus. He has served as a consultant to Genfit, Gilead, Malinckrodt, Pfizer, Salix, Boehringer Ingelheim, Novartis, Bristol Myers Squibb, Merck, Hemoshear, Lilly, Novo Nordisk, Terns, Albireo, Janssen, Poxel, 89bio, Siemens, AstraZeneca, NGM Bio, Amgen, Regeneron, Genentech, Alnylam, Roche, Madrigal, Inventiva, Covance, Prosciento, Histoindex, and PathAI. His institution has received grant support from Gilead, Malinckrodt, Boehringer Ingelheim, Novartis, Bristol Myers Squibb, Merck, Lilly, Novo Nordisk, Fractyl, Madrigal, and Inventiva. He has received royalties from Elsevier and UptoDate. PNN has received grants from Novo Nordisk and Boehringer Ingelheim; and has acted as a consultant on behalf of the University of Birmingham for Novo Nordisk, Boehringer Ingelheim, Gilead, Intercept Pharmaceuticals, Pfizer, and Poxel Pharmaceuticals. VR has acted as a consultant for Boehringer Ingelheim, Novo Nordisk, Poxel, Enyo, Madrigal, Terns, Intercept, NGM Bio, and Pfizer; and received research grants from Gilead Sciences and Intercept Pharmaceuticals.
Figures
Comment in
-
Semaglutide in NASH-related cirrhosis: too late to the party?Lancet Gastroenterol Hepatol. 2023 Jun;8(6):494-495. doi: 10.1016/S2468-1253(23)00069-9. Epub 2023 Mar 16. Lancet Gastroenterol Hepatol. 2023. PMID: 36934739 No abstract available.
-
Semaglutide in NASH-related cirrhosis: still a long way to go?Lancet Gastroenterol Hepatol. 2023 Aug;8(8):694. doi: 10.1016/S2468-1253(23)00109-7. Lancet Gastroenterol Hepatol. 2023. PMID: 37453428 No abstract available.
References
-
- Taylor RS, Taylor RJ, Bayliss S, et al. Association between fibrosis stage and outcomes of patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterology 2020; 158: 1611–25. - PubMed
-
- Mantovani A, Csermely A, Petracca G, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2021; 6: 903–13. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
