

A predictive model of polymetastatic disease from a multicenter large retrospectIve database on colorectal lung metastases treated with stereotactic ablative radiotherapy: The RED LaIT-SABR study
- PMID: 36935855
- PMCID: PMC10014322
- DOI: 10.1016/j.ctro.2022.100568
A predictive model of polymetastatic disease from a multicenter large retrospectIve database on colorectal lung metastases treated with stereotactic ablative radiotherapy: The RED LaIT-SABR study
Abstract
Aim: Stereotactic ablative radiotherapy (SABR) showed increasing survival in oligometastatic patients. Few studies actually depicted oligometastatic disease (OMD) evolution and which patient will remain disease-free and which will rapidly develop a polymetastatic disease (PMD) after SABR. Therefore, apart from the number of active metastases, there are no clues on which proven factor should be considered for prescribing local treatment in OMD. The study aims to identify predictive factors of polymetastatic evolution in lung oligometastatic colorectal cancer patients.
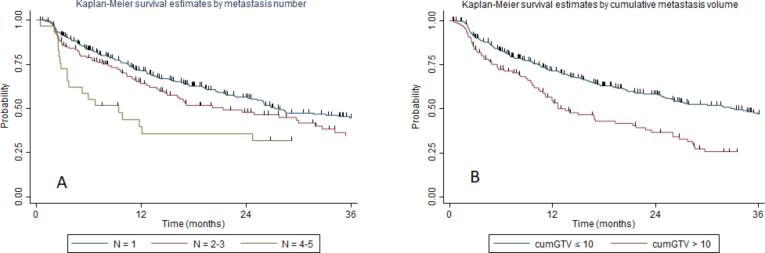
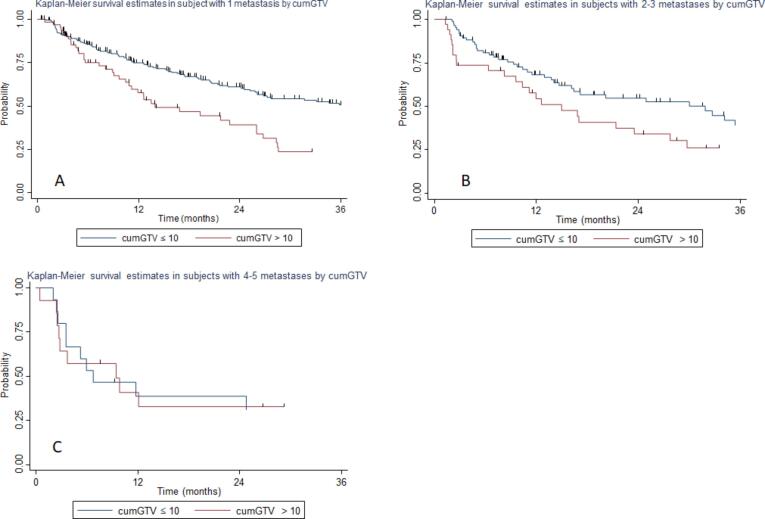
Methods: This international Ethical Committee approved trial (Prot. Negrar 2019-ZT) involved 23 Centers and 450 lung oligometastatic patients. Primary end-point was time to the polymetastatic conversion (tPMC). Additionally, oligometastases number and cumulative gross tumor volume (cumGTV) were used as combined predictive factors of tPMC. Oligometastases number was stratified as 1, 2-3, and 4-5; cumGTV was dichotomized to the value of 10 cc.
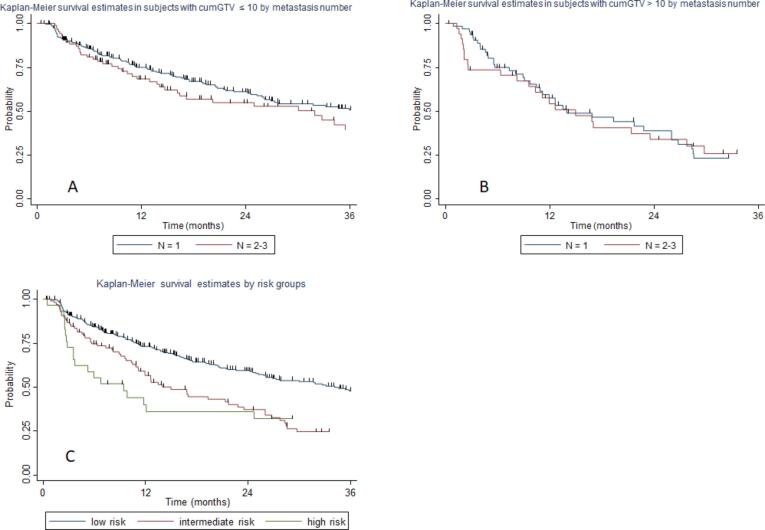
Results: The median tPMC in the overall population was 26 months. Population was classified in the following tPMC risk classes: low-risk (1-3 oligometastases and cumGTV ≤ 10 cc) with median tPMC of 35.1 months; intermediate-risk (1-3 oligometastases and cumGTV > 10 cc), with median tPMC of 13.9 months, and high-risk (4-5 oligometastases, any cumGTV) with median tPMC of 9.4 months (p = 0.000).
Conclusion: The present study identified predictive factors of polymetastatic evolution after SABR in lung oligometastatic colorectal cancer. The results demonstrated that the sole metastases number is not sufficient to define the OMD since patients defined oligometastatic from a numerical point of view might rapidly progress to PMD when the cumulative tumor volume is high. A tailored approach in SABR prescription should be pursued considering the expected disease evolution after SABR, with the aim to avoid unnecessary treatment and toxicity in those at high risk of polymetastatic spread, and maximize local treatment in those with a favorable disease evolution.
Keywords: Colorectal cancer; Oligometastatic disease; Predictive factors; SABR; SBRT; Stereotactic ablative radiotherapy.
© 2022 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Ost P., Reynders D., Decaestecker K., Fonteyne V., Lumen N., De Bruycker A., et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018;36(5):446–453. - PubMed
-
- Nicosia L., Figlia V., Ricottone N., Cuccia F., Mazzola R., Giaj-Levra N., et al. Stereotactic body radiotherapy (SBRT) and concomitant systemic therapy in oligoprogressive breast cancer patients [published online ahead of print, 2022 May 5] Clin Exp Metastasis. 2022;39(4):581–588. - PubMed
-
- Lievens Y., Guckenberger M., Gomez D., Hoyer M., Iyengar P., Kindts I., et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother Oncol. 2020;148:157–166. - PubMed
LinkOut - more resources
Full Text Sources
