

Case report: Acinetobacter baumannii septic arthritis in an immunocompetent infant
- PMID: 36936223
- PMCID: PMC10014783
- DOI: 10.3389/fmed.2023.1135178
Case report: Acinetobacter baumannii septic arthritis in an immunocompetent infant
Abstract
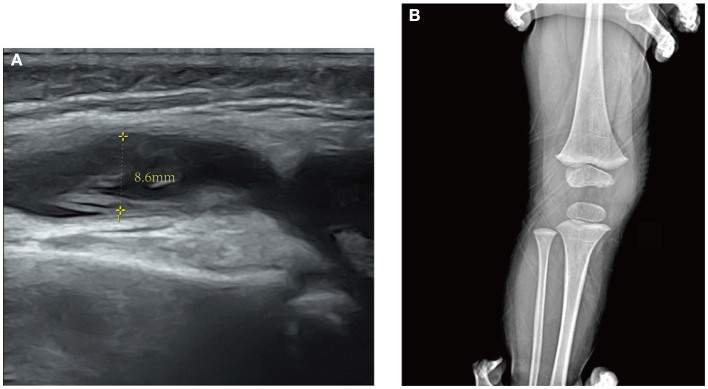
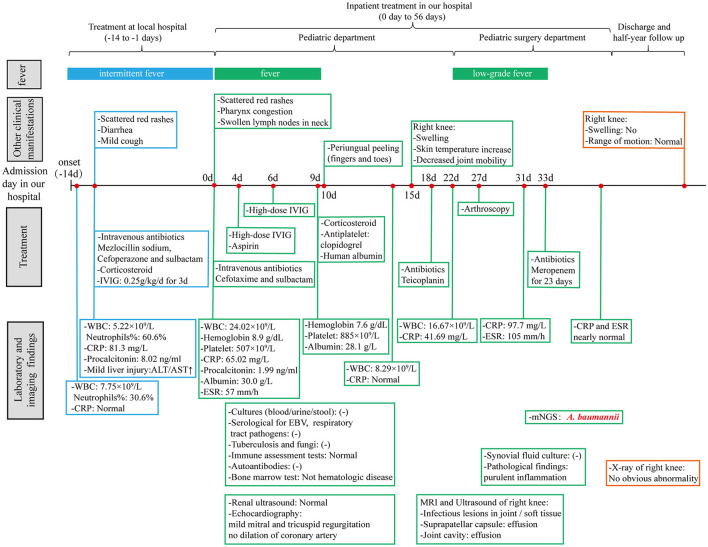
Acinetobacter baumannii is a gram-negative coccobacilli, mainly causing nosocomial infections with poor prognosis, especially in patients with prolonged hospitalization or antibiotics administration. A. baumannii pneumonia is the most common clinical form and usually occurs in critically ill patients in the intensive care unit. However, septic arthritis caused by A. baumannii is rarely reported. In this report, we describe a case of A. baumannii septic arthritis combined with incomplete Kawasaki disease in an infant. The child's chief complaint was a 2-week intermittent fever with poor response to antibiotics. Initial physical examination revealed swollen lymph nodes in the neck, pharynx congestion, and the appearance of rashes. Combined with laboratory tests, the diagnosis of incomplete Kawasaki disease was considered. After administration of high-dose intravenous immunoglobulin and corticosteroids, the child's fever improved and periungual desquamation appeared simultaneously. Swelling of the right knee occurred 5 days after the fever improved and imaging tests of MRI and ultrasound suggested the existence of infection. A diagnosis of septic arthritis was established subsequently, and arthroscopy was carried out. A. baumannii was finally identified by metagenomics next-generation sequencing of joint draining fluid for pathogenic microorganisms. Treatment with meropenem was then started. The patient eventually recovered and was discharged from the hospital after 23 days of treatment with meropenem. Although A. baumannii is not a common bacterium of septic arthritis, this rare infection can still occur in infants. Early diagnosis, pathogenic identification, and target antibiotic treatment are important to reduce the occurrence of joint sequelae.
Keywords: Acinetobacter baumannii; case report; infant; metagenomics next-generation sequencing; septic arthritis.
Copyright © 2023 Liao, Xiao, Fang, Zhou, Liu and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources