

Severity of maternal infection and perinatal outcomes during periods of SARS-CoV-2 wildtype, alpha, and delta variant dominance in the UK: prospective cohort study
- PMID: 36936566
- PMCID: PMC9978672
- DOI: 10.1136/bmjmed-2021-000053
Severity of maternal infection and perinatal outcomes during periods of SARS-CoV-2 wildtype, alpha, and delta variant dominance in the UK: prospective cohort study
Abstract
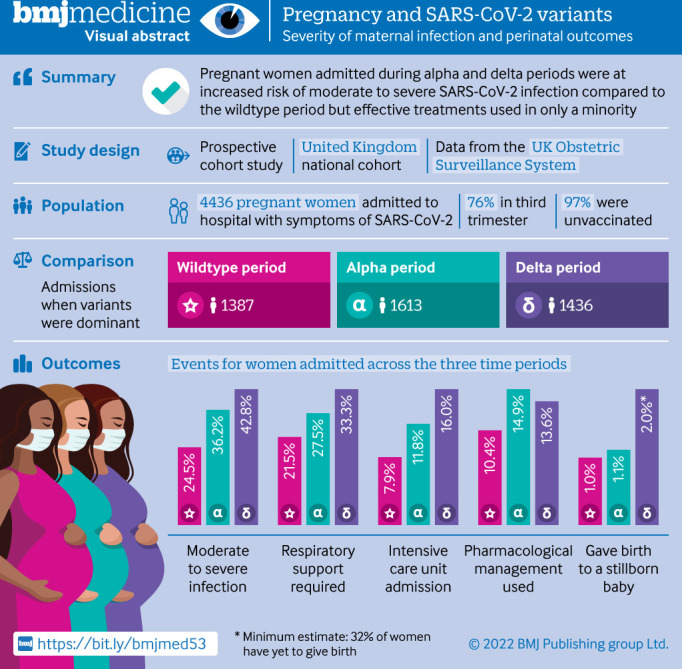
Objective: To compare the severity of maternal infection and perinatal outcomes during periods in which wildtype, alpha variant, and delta variant of SARS-CoV-2 were dominant in the UK.
Design: Prospective cohort study.
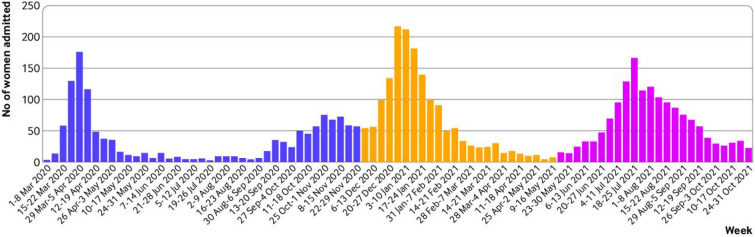
Setting: 194 obstetric units across the UK, during the following periods: between 1 March and 30 November 2020 (wildtype dominance), between 1 December 2020 and 15 May 2021 (alpha variant dominance), and between 16 May and 31 October 2021 (delta variant dominance).
Participants: 4436 pregnant women admitted to hospital with covid-19 related symptoms.
Main outcome measures: Moderate to severe maternal SARS-CoV-2 infection (indicated by any of the following: oxygen saturation <95% on admission, need for oxygen treatment, evidence of pneumonia on imaging, admission to intensive care, or maternal death), and pregnancy and perinatal outcomes (including mode and gestation of birth, stillbirth, live birth, admission to neonatal intensive care, and neonatal death).
Results: 1387, 1613, and 1436 pregnant women were admitted to hospital with covid-19 related symptoms during the wildtype, alpha, and delta dominance periods, respectively; of these women, 340, 585, and 614 had moderate to severe infection, respectively. The proportion of pregnant women admitted with moderate to severe infection increased during the subsequent alpha and delta dominance periods, compared with the wildtype dominance period (wildtype 24.5% v alpha 36.2% (adjusted odds ratio 1.98, 95% confidence interval 1.66% to 2.37%); wildtype 24.5% v delta 42.8% (2.66, 2.21 to 3.20)). Compared with the wildtype dominance period, women admitted during the alpha dominance period were significantly more likely to have pneumonia, require respiratory support, and be admitted to intensive care; these three risks were even greater during the delta dominance period (wildtype v delta: pneumonia, adjusted odds ratio 2.52, 95% confidence interval 2.06 to 3.09; respiratory support, 1.90, 1.52 to 2.37; and intensive care, 2.71, 2.06 to 3.56). Of 1761 women whose vaccination status was known, 38 (2.2%) had one dose and 16 (1%) had two doses before their diagnosis (of whom 14 (88%) had mild infection). The proportion of women receiving drug treatment for SARS-CoV-2 management was low, but did increase between the wildtype dominance period and the alpha and delta dominance periods (10.4% wildtype v 14.9% alpha (2.74, 2.08 to 3.60); 10.4% wildtype v 13.6% delta (2.54, 1.90 to 3.38)).
Conclusions: While limited by the absence of variant sequencing data, these findings suggest that during the periods when the alpha and delta variants of SARS-CoV-2 were dominant, covid-19 was associated with more severe maternal infection and worse pregnancy outcomes than during the wildtype dominance period. Most women admitted with SARS-CoV-2 related symptoms were unvaccinated. Urgent action to prioritise vaccine uptake in pregnancy is essential.
Study registration: ISRCTN40092247.
Keywords: COVID-19; neonatology; pregnancy complications.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: MK, MQ, PB, PO’B, and JJK received grants from the NIHR in relation to the submitted work; KB, NV, and NABS declare no conflicts of interest; EM is trustee of the Royal College of Obstetricians and Gynaecologists and British Menopause Society, and new chair of the board of trustees for Group B Strep Support; CG was financially supported by UK Medical Research Council (MRC)through a clinician scientist fellowship; PB was past chair of the MRC/NIHR Methodology Research Programme panel with previous grant funding from MRC, NIHR, and the Welcome Trust, and provides consultancy services for personal fees to AG Biotest.
Figures
References
-
- World Health Organisation . Tracking SARS-CoV-2 variants. Geneva: World Health Organisation, 2021. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
-
- Public Health England . SARS-CoV-2 variants of concern and variants under investigation in England: technical Briefing 13. London: Public Health England, 2021.
LinkOut - more resources
Full Text Sources
Miscellaneous