

Impact of severe secondary tricuspid regurgitation on rest and exercise hemodynamics of patients with heart failure and a preserved left ventricular ejection fraction
- PMID: 36937944
- PMCID: PMC10014840
- DOI: 10.3389/fcvm.2023.1061118
Impact of severe secondary tricuspid regurgitation on rest and exercise hemodynamics of patients with heart failure and a preserved left ventricular ejection fraction
Abstract
Background: Both secondary tricuspid regurgitation (STR) and heart failure with preserved ejection fraction (HFpEF) are relevant public health problems in the elderly population, presenting with potential overlaps and sharing similar risk factors. However, the impact of severe STR on hemodynamics and cardiorespiratory adaptation to exercise in HFpEF remains to be clarified.
Aim: To explore the impact of STR on exercise hemodynamics and cardiorespiratory adaptation in HFpEF.
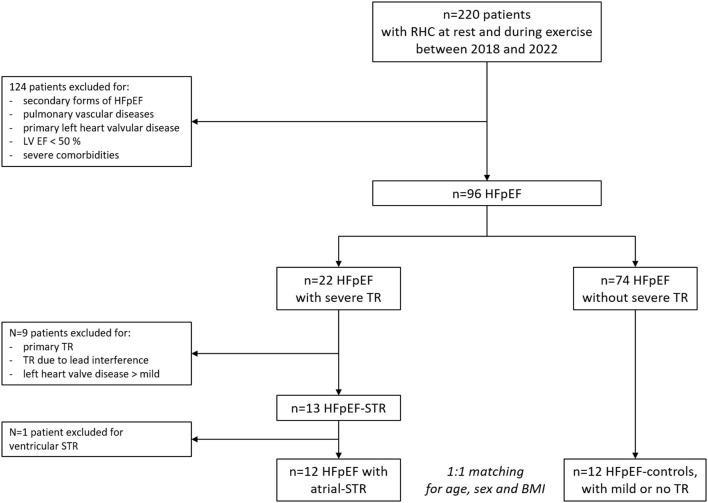
Methods: We analyzed invasive hemodynamics and gas-exchange data obtained at rest and during exercise from HFpEF patients with severe STR (HFpEF-STR), compared with 1:1 age-, sex-, and body mass index (BMI)- matched HFpEF patients with mild or no STR (HFpEF-controls).
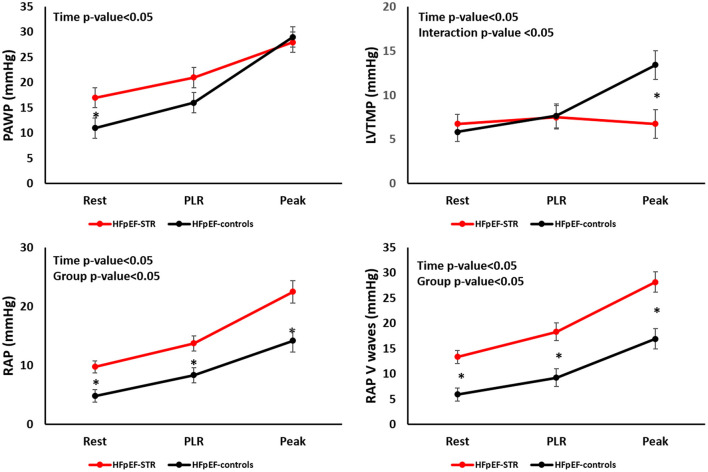
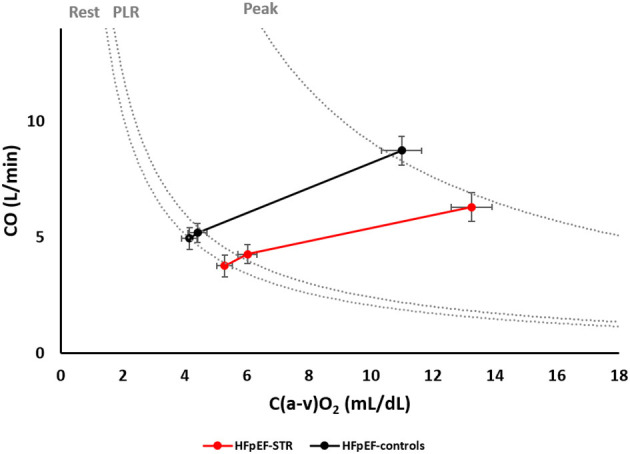
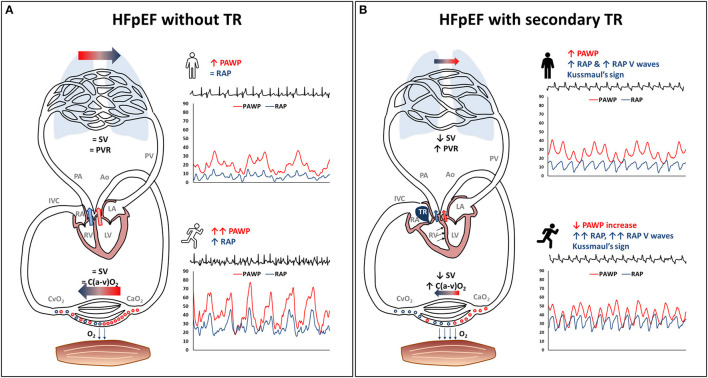
Results: Twelve HFpEF with atrial-STR (mean age 72 years, 92% females, BMI 28 Kg/m2) and 12 HFpEF-controls patients were analyzed. HFpEF-STR had higher (p < 0.01) right atrial pressure than HFpEF-controls both at rest (10 ± 1 vs. 5 ± 1 mmHg) and during exercise (23 ± 2 vs. 14 ± 2 mmHg). Despite higher pulmonary artery wedge pressure (PAWP) at rest in HFpEF-STR than in HFpEF-controls (17 ± 2 vs. 11 ± 2, p = 0.04), PAWP at peak exercise was no more different (28 ± 2 vs. 29 ± 2). Left ventricular transmural pressure and cardiac output (CO) increased less in HFpEF-STR than in HFpEF-controls (interaction p-value < 0.05). This latter was due to lower stroke volume (SV) values both at rest (48 ± 9 vs. 77 ± 9 mL, p < 0.05) and at peak exercise (54 ± 10 vs. 93 ± 10 mL, p < 0.05). Despite these differences, the two groups of patients laid on the same oxygen consumption isophlets because of the increased peripheral oxygen extraction in HFpEF-STR (p < 0.01). We found an inverse relationship between pulmonary vascular resistance and SV, both at rest and at peak exercise (R 2 = 0.12 and 0.19, respectively).
Conclusions: Severe STR complicating HFpEF impairs SV and CO reserve, leading to pulmonary vascular de-recruitment and relative left heart underfilling, undermining the typical HFpEF pathophysiology.
Keywords: exercise; heart failure with preserved ejection faction; hemodynamics; oxygen consumption; right heart catheterization; tricuspid regurgitation.
Copyright © 2023 Baratto, Caravita, Corbetta, Soranna, Zambon, Dewachter, Gavazzoni, Heilbron, Tomaselli, Radu, Perelli, Perego, Vachiéry, Parati, Badano and Muraru.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer GI declared a shared parent affiliation with the authors CB, SC, GC, DS, AZ, MG, FH, MT, NR, FP, GPe, GPa, LB, and DM to the handling editor at the time of the review.
Figures
References
LinkOut - more resources
Full Text Sources