

TACE and conformal radiotherapy vs. TACE alone for hepatocellular carcinoma: A randomised controlled trial
- PMID: 36937990
- PMCID: PMC10017427
- DOI: 10.1016/j.jhepr.2023.100689
TACE and conformal radiotherapy vs. TACE alone for hepatocellular carcinoma: A randomised controlled trial
Abstract
Background & aims: Transcatheter arterial chemoembolisation (TACE) is recommended for patients with hepatocellular carcinoma devoid of macrovascular invasion or extrahepatic spread but not eligible for curative therapies. We compared the efficacy and safety of the combination of a single TACE and external conformal radiotherapy (CRT) vs. classical TACE.
Methods: TACERTE was an open-labelled, randomised controlled trial with a 1:1 allocation rate to two or three TACE (arm A) or one TACE + CRT (arm B). Participants had a mean age of 70 years, and 86% were male. The aetiology was alcohol in 85%. The primary endpoint was liver progression-free survival (PFS) in the intention-to-treat population. The typical CRT schedule was 54 Gy in 18 sessions of 3 Gy.
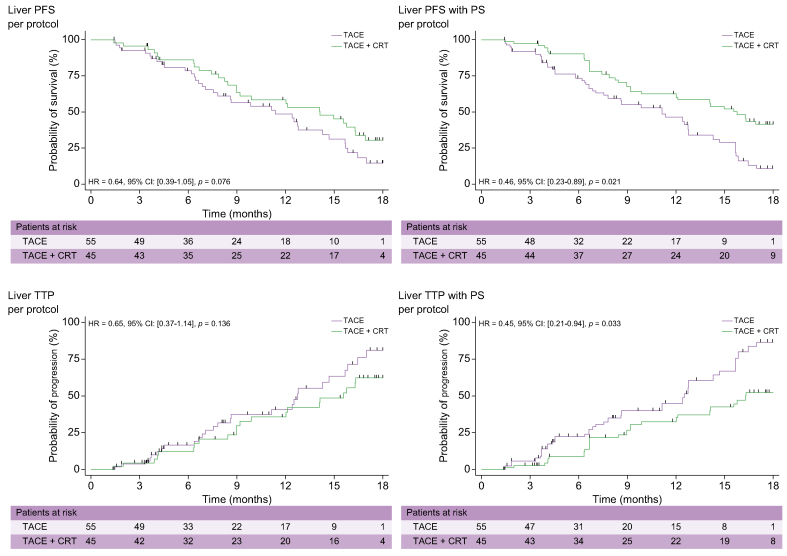
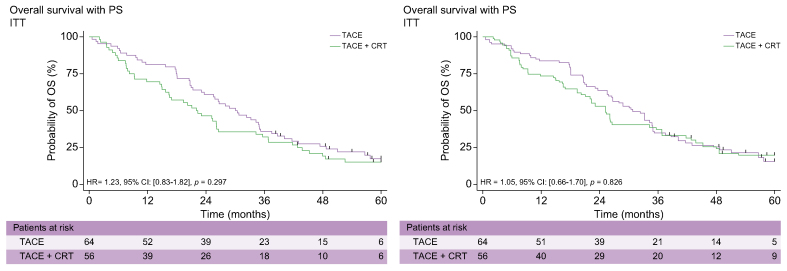
Results: Of the 120 participants randomised, 64 were in arm A and 56 in arm B; 100 participants underwent the planned schedule and defined the 'per-protocol' group. In intention-to-treat participants, the liver PFS at 12 and 18 months were 59% and 19% in arm A and 61% and 36% in arm B (hazard ratio [HR] 0.69; 95% CI 0.40-1.18; p = 0.17), respectively. In the per-protocol population, treated liver PFS tended to be better in arm B (HR 0.61; 95% CI 0.34-1.06; p = 0.081) than in arm A. Liver-related grade III-IV adverse events were more frequent in arm B than in arm A. Median overall survival reached 30 months (95% CI 23-35) in arm A and 22 months (95% CI 15.7-26.2) in arm B.
Conclusions: Although TACE + CRT tended to improve local control, this first Western randomised controlled trial showed that the combined strategy failed to increase PFS or overall survival and led more frequently to liver-related adverse effects.
Impact and implications: Hepatocellular carcinoma is frequently treated by arterial embolisation of the tumour and more recently by external radiotherapy. We tried to determine whether combination of the two treatments (irradiation after embolisation) might produce interesting results. Our results in this prospective randomised study were not able to demonstrate a beneficial effect of combining embolisation and irradiation in these patients. On the contrary, we observed more adverse effects with the combined treatment.
Clinical trials registration: NCT01300143.
Keywords: 3-DCRT, three-dimensional conformal radiotherapy; AE, adverse event; ALBI, albumin–bilirubin; BCLC, Barcelona Clinic Liver Cancer; CRT, conformal radiotherapy; CT, computed tomography; CTV, clinical tumour volume; Conformal external radiotherapy; ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; HR, hazard ratio; Hepatocellular carcinoma; ITT, intention-to-treat; OS, overall survival; PFS, progression-free survival; PS, propensity score; RILD, radio-induced liver disease; SBRT, stereotaxic body radiation therapy; TACE, transcatheter arterial chemoembolisation; TTP, time to tumour progression; mRECIST, modified Response Evaluation Criteria in Solid Tumour.
© 2023 The Authors.
Conflict of interest statement
CF, LC, IA, XM, ER, CP, LM, FO, YT, JG, HR, JE, AR, PH, JFB, ENK, DA, AGP, EF-P, and HA did not receive any grants or funding. P Merle reports grants or funding from Roche, AstraZeneca, MSD, Eisai, Bayer, and Ipsen. P Mathurin reports grants or funding from Ipsen, Eisai, Abbvie, Sanofi, Gilead Sciences, Pfizer, Evive Biotech, Novo Nordisk, Bayer Healthcare, Surrozen, and Intercept. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures




References
-
- Llovet J.M., Brú C., Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19:329–338. - PubMed
-
- European Association for the Study of the Liver EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. - PubMed
-
- Huo Y.R., Eslick G.D. Transcatheter arterial chemoembolization plus radiotherapy compared with chemoembolization alone for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Oncol. 2015;1:756–765. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
