

Association of Longitudinal Urinary Metabolic Biomarkers With ADPKD Severity and Response to Metformin in TAME-PKD Clinical Trial Participants
- PMID: 36938071
- PMCID: PMC10014337
- DOI: 10.1016/j.ekir.2022.11.019
Association of Longitudinal Urinary Metabolic Biomarkers With ADPKD Severity and Response to Metformin in TAME-PKD Clinical Trial Participants
Abstract
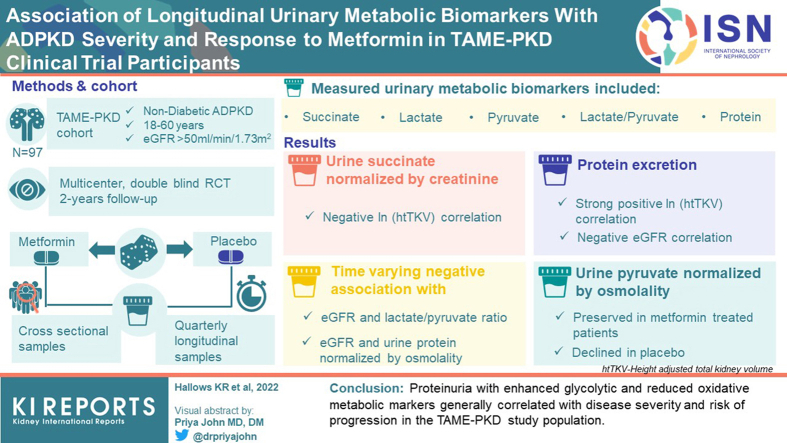
Introduction: Dysregulated cellular metabolism contributes to autosomal dominant polycystic kidney disease (ADPKD) pathogenesis. The Trial of Administration of Metformin in Polycystic Kidney Disease (TAME-PKD) tested the effects of metformin treatment over 2 years in adult ADPKD patients with mild-moderate disease severity. Metformin was found to be safe and tolerable with an insignificant trend toward reduced estimated glomerular filtration rate (eGFR) decline compared to placebo. Here we tested whether targeted urinary metabolic biomarkers measured in TAME-PKD participants correlated with disease progression, severity, and metformin treatment in cross-sectional and longitudinal analyses.
Methods: Concentrations of total protein, targeted metabolites (lactate, pyruvate, and succinate), and glycolytic enzymes (pyruvate kinase-M2, lactate dehydrogenase-A, and pyruvate dehydrogenase kinase-1) were measured and normalized by creatinine or osmolality in urine specimens and compared with height-adjusted total kidney volume (htTKV) and eGFR at the different study timepoints.
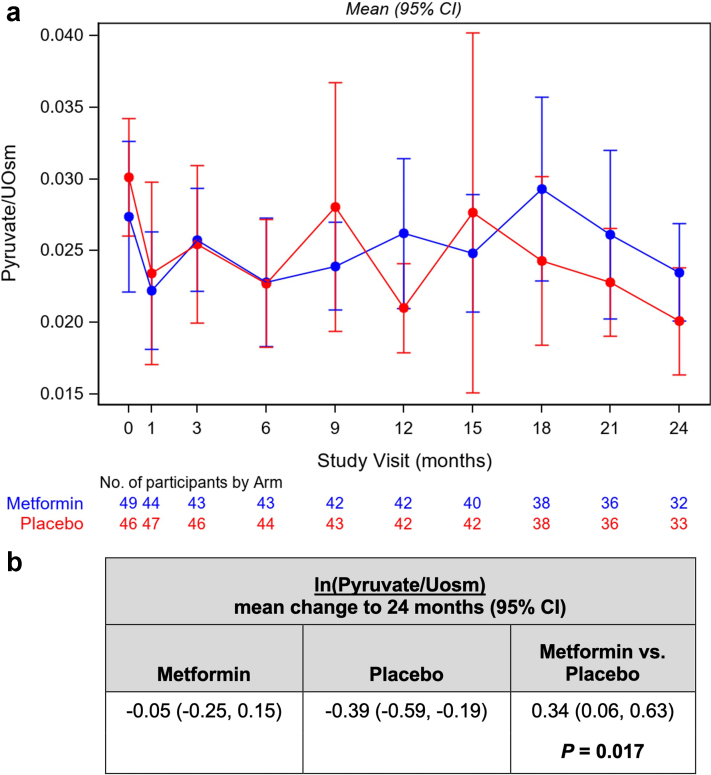
Results: In cross-sectional analyses utilizing placebo group data, urinary succinate normalized by creatinine negatively correlated with ln (htTKV), whereas protein excretion strongly positively correlated with ln (htTKV), and negatively correlated with eGFR. Significant time-varying negative associations occurred with eGFR and the lactate/pyruvate ratio and with urine protein normalized by osmolality, indicating correlations of these biomarkers with disease progression. In secondary analyses, urinary pyruvate normalized by osmolality was preserved in metformin-treated participants but declined in placebo over the 2-year study period with a significant between-arm difference, suggesting time-dependent urinary pyruvate changes may serve as a discriminator for metformin treatment effects in this study population.
Conclusion: Proteinuria with enhanced glycolytic and reduced oxidative metabolic markers generally correlated with disease severity and risk of progression in the TAME-PKD study population.
Keywords: ADPKD; biomarkers; eGFR; metformin; proteinuria.
© 2022 Published by Elsevier Inc. on behalf of the International Society of Nephrology.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
