

Clinical symptoms and immune injury reflected by low CD4/CD8 ratio should increase the suspicion of HIV coinfection with tuberculosis
- PMID: 36938418
- PMCID: PMC10015191
- DOI: 10.1016/j.heliyon.2023.e14219
Clinical symptoms and immune injury reflected by low CD4/CD8 ratio should increase the suspicion of HIV coinfection with tuberculosis
Abstract
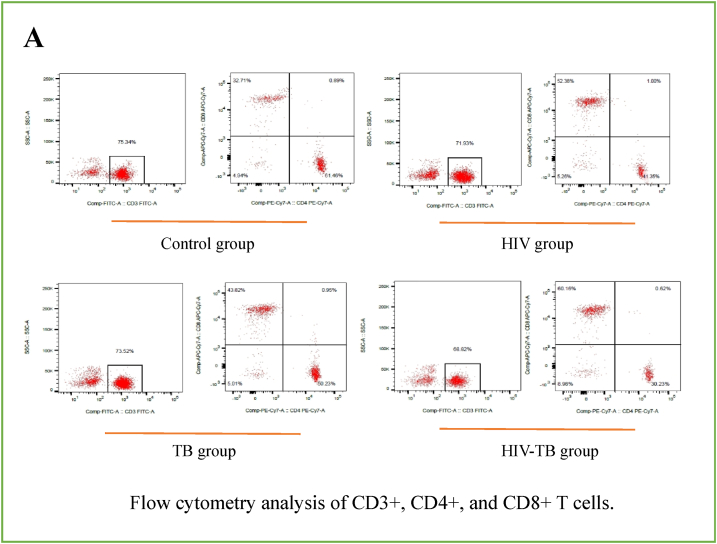
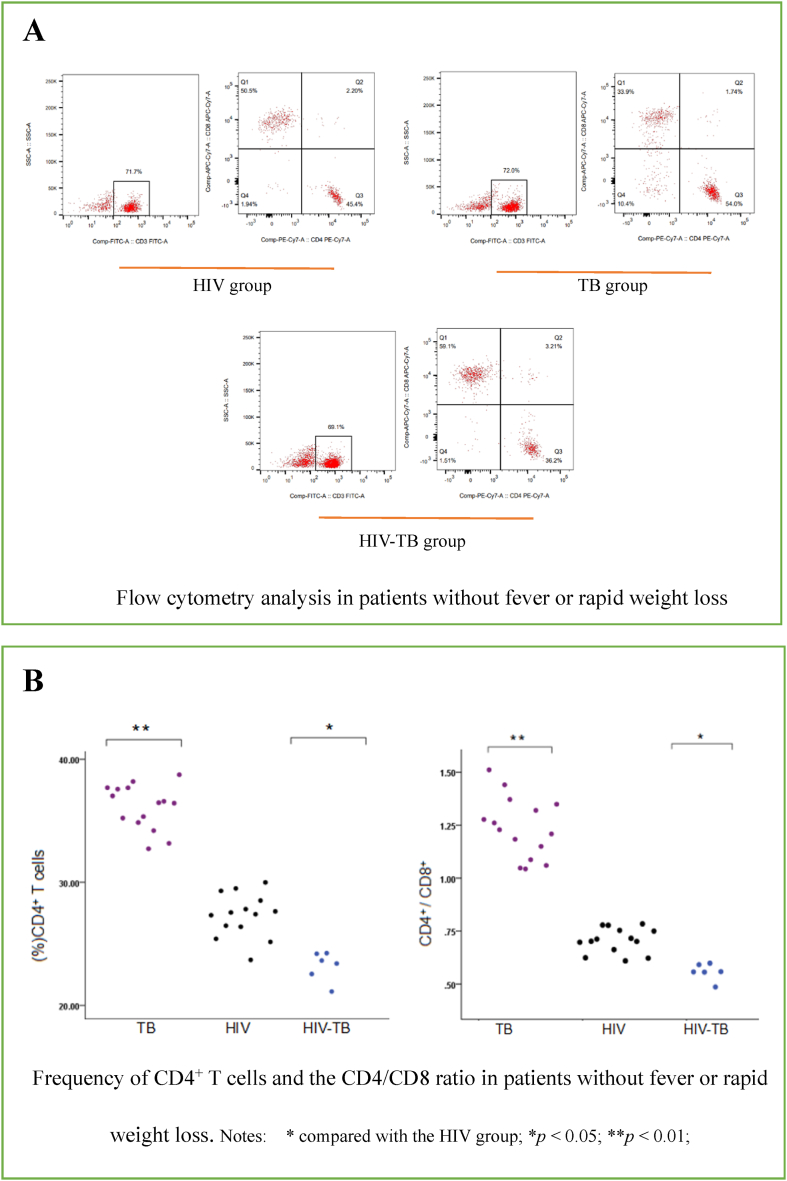
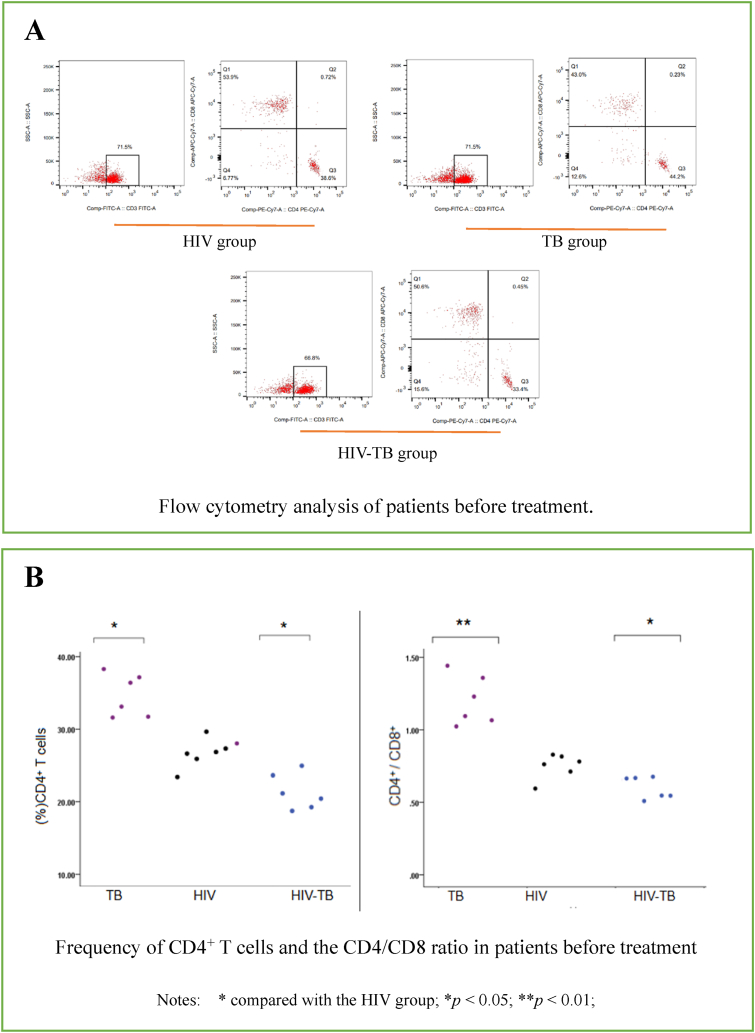
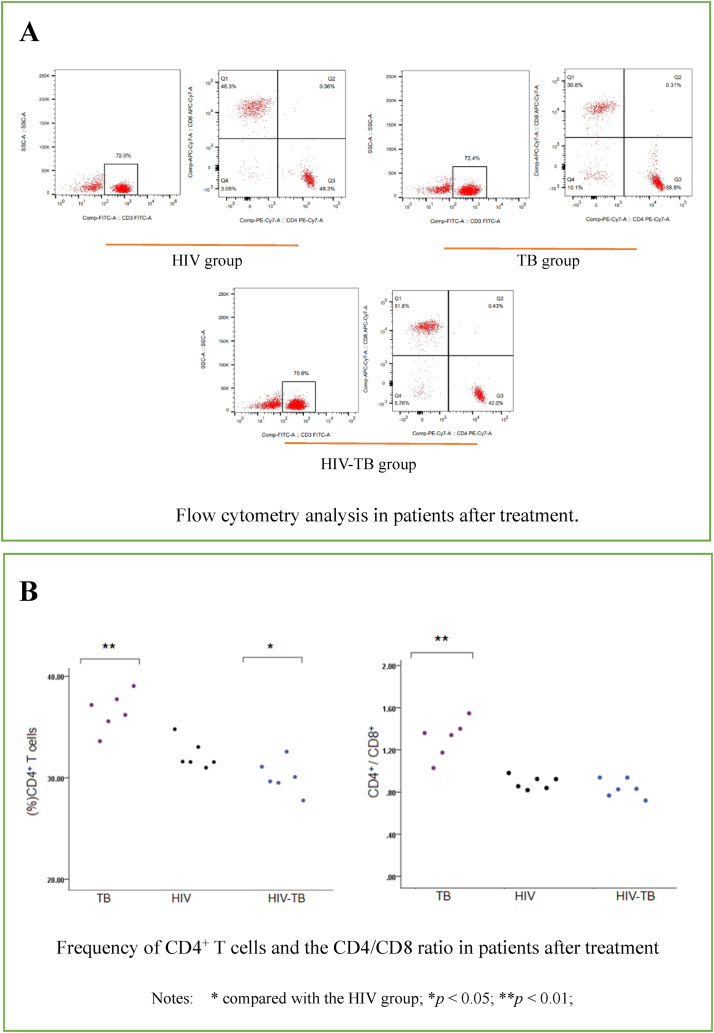
Background: Patients who are coinfected with human immunodeficiency virus 1 (HIV) and Mycobacterium tuberculosis (TB) benefit from timely diagnosis and treatment. In the present study frequencies of CD3+, CD4+, and CD8+ T cells among peripheral blood mononuclear cells (PBMCs) of patients in the Kashi region of China infected with HIV, TB, and both HIV and TB (HIV-TB) were investigated to provide a basis for rapid identification of coinfected patients.
Methods: A total of 62 patients with HIV, TB, or HIV-TB who were first hospitalized at our institution were included in the study, as were 30 controls. PBMCs were isolated, and the frequencies of CD3+, CD4+, and CD8+ T cells were determined via flow cytometry.
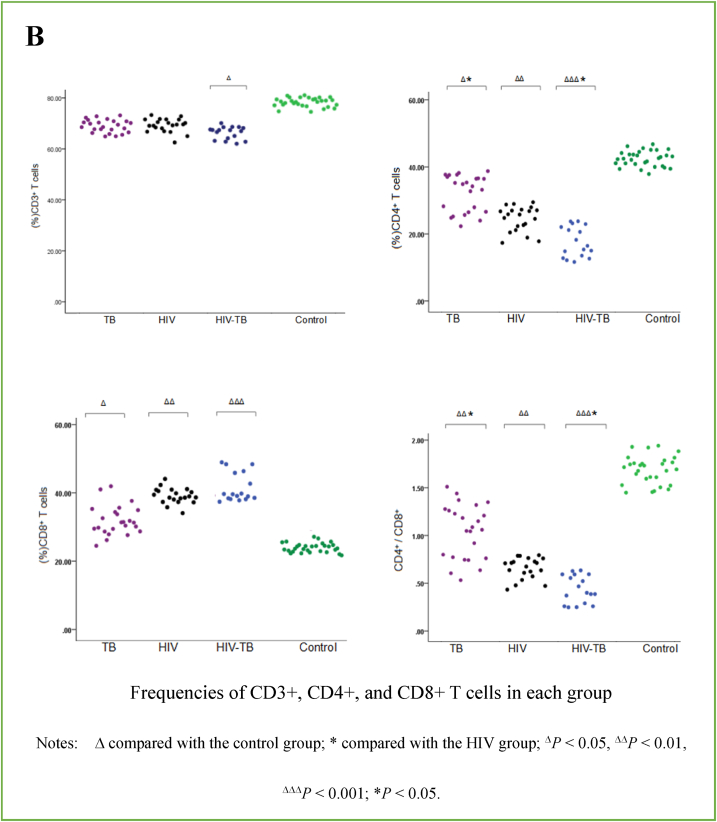
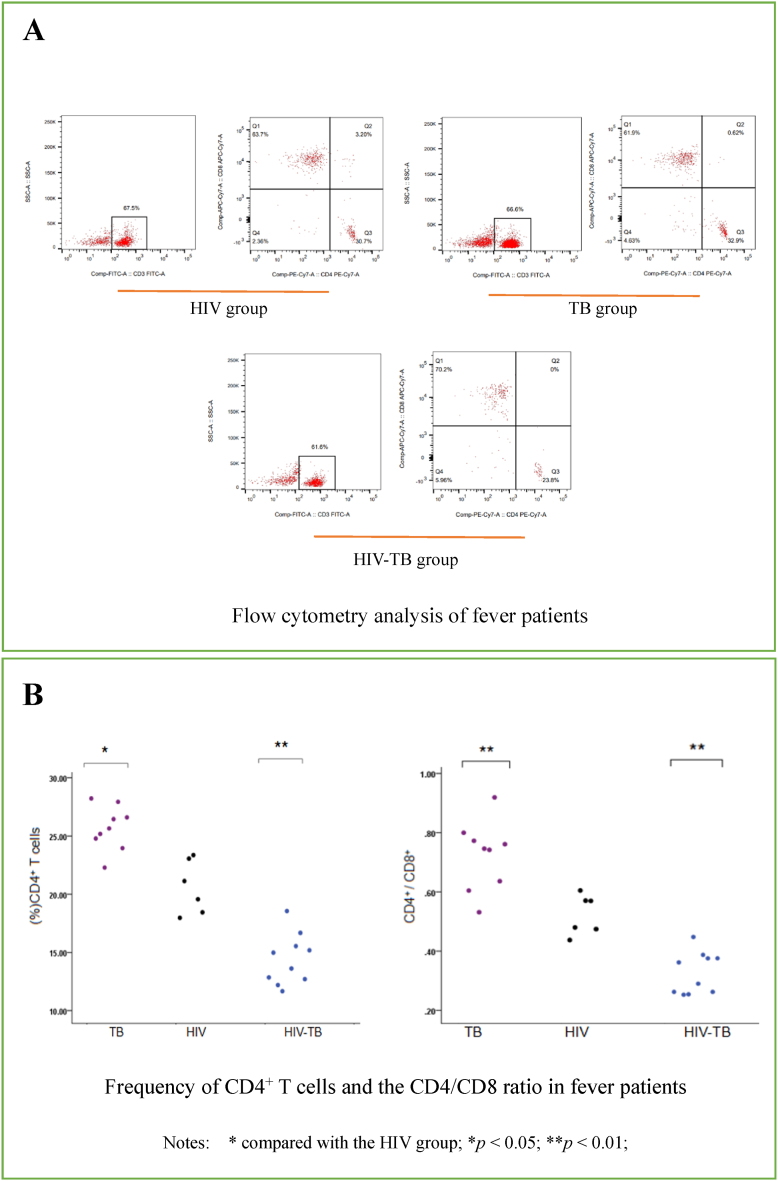
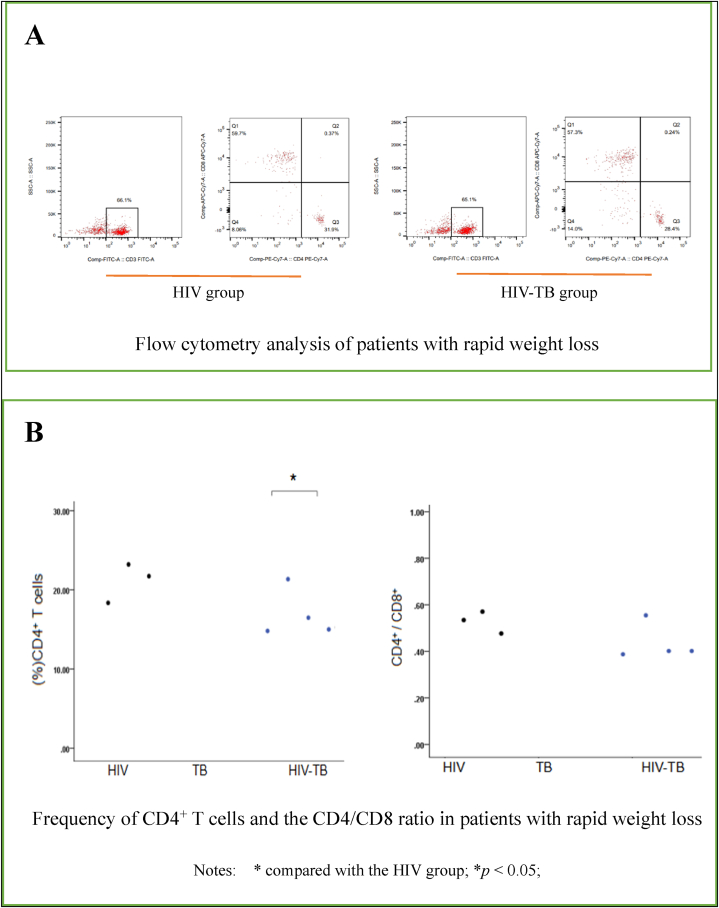
Results: The frequency of CD4+ T cells and the CD4/CD8 ratio were significantly lower in the HIV-TB group than in the other three groups. In fever patients the frequency of CD4+ T cells and the CD4/CD8 ratio were significantly lower in the HIV-TB group than in the HIV group and the TB group. In patients who exhibited rapid weight loss there were no significant differences in the frequency of CD4+ T cells or the CD4/CD8 ratio between the groups. The results of treatment were compared in the HIV, TB, and HIV-TB groups after 7 days, and there were obvious improvements in the frequency of CD4+ T cells and the CD4/CD8 ratio.
Conclusion: Clinical symptoms and the degree of immune injury can heighten suspicion for HIV-TB coinfection.
Keywords: CD4+ T cells; CD4/CD8 ratio; HIV-TB coinfection.
© 2023 The Authors.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Badri M., Ehrlich R., Wood R., et al. Association between tuberculosis and HIV disease progression in a high tuberculosis prevalence area. Int. J. Tubercul. Lung Dis. 2001;5:225–232. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
