

Exploring Digital Biomarkers of Illness Activity in Mood Episodes: Hypotheses Generating and Model Development Study
- PMID: 36939345
- PMCID: PMC10196899
- DOI: 10.2196/45405
Exploring Digital Biomarkers of Illness Activity in Mood Episodes: Hypotheses Generating and Model Development Study
Abstract
Background: Depressive and manic episodes within bipolar disorder (BD) and major depressive disorder (MDD) involve altered mood, sleep, and activity, alongside physiological alterations wearables can capture.
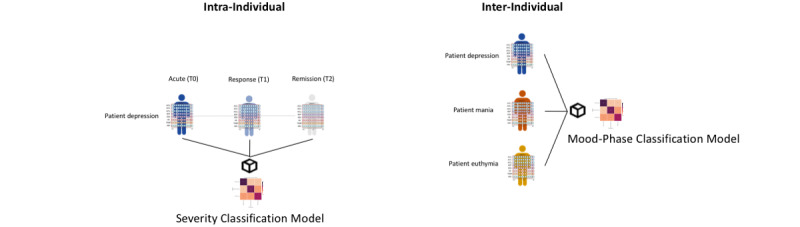
Objective: Firstly, we explored whether physiological wearable data could predict (aim 1) the severity of an acute affective episode at the intra-individual level and (aim 2) the polarity of an acute affective episode and euthymia among different individuals. Secondarily, we explored which physiological data were related to prior predictions, generalization across patients, and associations between affective symptoms and physiological data.
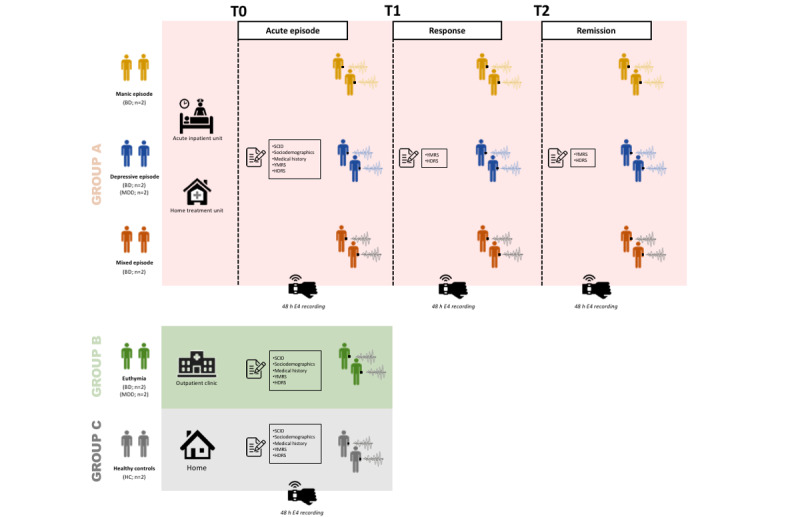
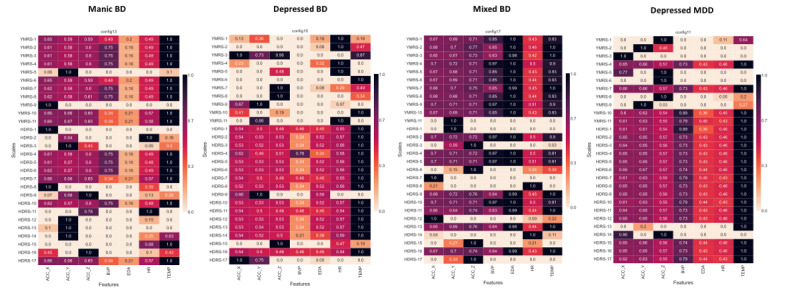
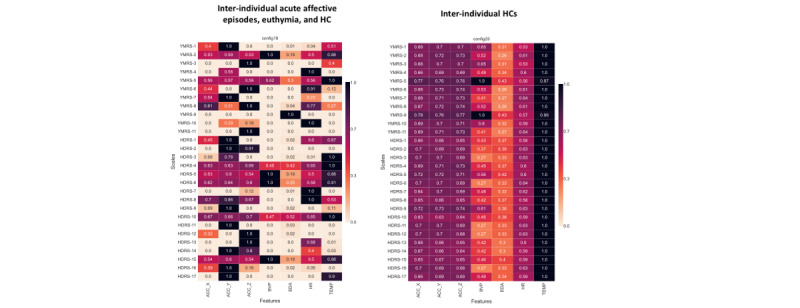
Methods: We conducted a prospective exploratory observational study including patients with BD and MDD on acute affective episodes (manic, depressed, and mixed) whose physiological data were recorded using a research-grade wearable (Empatica E4) across 3 consecutive time points (acute, response, and remission of episode). Euthymic patients and healthy controls were recorded during a single session (approximately 48 h). Manic and depressive symptoms were assessed using standardized psychometric scales. Physiological wearable data included the following channels: acceleration (ACC), skin temperature, blood volume pulse, heart rate (HR), and electrodermal activity (EDA). Invalid physiological data were removed using a rule-based filter, and channels were time aligned at 1-second time units and segmented at window lengths of 32 seconds, as best-performing parameters. We developed deep learning predictive models, assessed the channels' individual contribution using permutation feature importance analysis, and computed physiological data to psychometric scales' items normalized mutual information (NMI). We present a novel, fully automated method for the preprocessing and analysis of physiological data from a research-grade wearable device, including a viable supervised learning pipeline for time-series analyses.
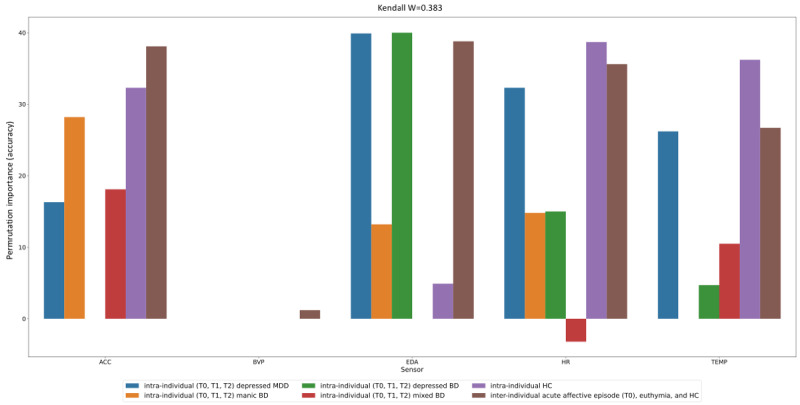
Results: Overall, 35 sessions (1512 hours) from 12 patients (manic, depressed, mixed, and euthymic) and 7 healthy controls (mean age 39.7, SD 12.6 years; 6/19, 32% female) were analyzed. The severity of mood episodes was predicted with moderate (62%-85%) accuracies (aim 1), and their polarity with moderate (70%) accuracy (aim 2). The most relevant features for the former tasks were ACC, EDA, and HR. There was a fair agreement in feature importance across classification tasks (Kendall W=0.383). Generalization of the former models on unseen patients was of overall low accuracy, except for the intra-individual models. ACC was associated with "increased motor activity" (NMI>0.55), "insomnia" (NMI=0.6), and "motor inhibition" (NMI=0.75). EDA was associated with "aggressive behavior" (NMI=1.0) and "psychic anxiety" (NMI=0.52).
Conclusions: Physiological data from wearables show potential to identify mood episodes and specific symptoms of mania and depression quantitatively, both in BD and MDD. Motor activity and stress-related physiological data (EDA and HR) stand out as potential digital biomarkers for predicting mania and depression, respectively. These findings represent a promising pathway toward personalized psychiatry, in which physiological wearable data could allow the early identification and intervention of mood episodes.
Keywords: Empatica E4; bipolar disorder; deep learning; depression; digital biomarker; machine learning; major depressive disorder; mania; physiological data; wearable.
©Gerard Anmella, Filippo Corponi, Bryan M Li, Ariadna Mas, Miriam Sanabra, Isabella Pacchiarotti, Marc Valentí, Iria Grande, Antoni Benabarre, Anna Giménez-Palomo, Marina Garriga, Isabel Agasi, Anna Bastidas, Myriam Cavero, Tabatha Fernández-Plaza, Néstor Arbelo, Miquel Bioque, Clemente García-Rizo, Norma Verdolini, Santiago Madero, Andrea Murru, Silvia Amoretti, Anabel Martínez-Aran, Victoria Ruiz, Giovanna Fico, Michele De Prisco, Vincenzo Oliva, Aleix Solanes, Joaquim Radua, Ludovic Samalin, Allan H Young, Eduard Vieta, Antonio Vergari, Diego Hidalgo-Mazzei. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org), 04.05.2023.
Conflict of interest statement
Conflicts of Interest: GA has received continuing medical education (CME)–related honoraria or consulting fees from Janssen-Cilag, Lundbeck, Lundbeck and Otsuka, and Angelini. IP has received CME-related honoraria, or consulting fees from ADAMED, Janssen-Cilag, and Lundbeck. IG has received grants and served as consultant, advisor or CME speaker for the following identities: Angelini, Casen Recordati, Ferrer, Janssen Cilag, and Lundbeck, Lundbeck-Otsuka, Luye, SEI Healthcare. AG-P has received CME-related honoraria, or consulting fees from Janssen-Cilag, Lundbeck, Casen Recordati and Angelini. MC has received grants and served as consultant, advisor or CME speaker for the following entities: Lundbeck, Esteve, Pfizer. NA has received CME-related financing from Janssen-Cilag, Lundbeck, Adamed, Pfizer, Angelini and Boston Scientific. MB has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of has received honoraria from talks and/or consultancy of Adamed, Angelini, Casen-Recordati, Exeltis, Ferrer, Janssen, Lundbeck, Neuraxpharm, Otsuka, Pfizer and Sanofi. NV has received financial support for CME activities and travel funds from the following entities: Angelini, Janssen-Cilag, Lundbeck, Otsuka. SM has received CME-related honoraria, or consulting fees from Janssen-Cilag, Lundbeck, Lundbeck/Otsuka, and Angelini. A Murru has received grants and served as consultant, advisor or CME speaker for the following entities: Angelini, Idorsia, Lundbeck, Pfizer, Takeda. LS has received CME-related honoraria, or consulting fees from Boehringer -Ingelheim, Janssen, Lundbeck/Otsuka, Sanofi-Aventis. AHY has received honoraria for lectures and advisory boards for all major pharmaceutical companies with drugs used in affective and related disorders. EV has received research support from or served as consultant, adviser or speaker for AB-Biotics, Abbott, Abbvie, Adamed, Angelini, Biogen, Celon, Dainippon Sumitomo Pharma, Ferrer, Gedeon Richter, GH Research, Glaxo SmithKline, Janssen, Lundbeck, Organon, Otsuka, Rovi, Sage pharmaceuticals, Sanofi-Aventis, Shire, Sunovion, Takeda, and Viatris. DH-M has received CME-related honoraria and served as consultant for Abbott, Angelini, Ethypharm Digital Therapy and Janssen-Cilag. All authors report no financial or other relationship relevant to the subject of this article.
Figures
References
-
- COVID-19 Mental Disorders Collaborators Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021 Nov 06;398(10312):1700–12. doi: 10.1016/S0140-6736(21)02143-7. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(21)02143-7 S0140-6736(21)02143-7 - DOI - PMC - PubMed
