

Exercise-Induced Left Atrial Hypertension in Heart Failure With Preserved Ejection Fraction
- PMID: 36939661
- PMCID: PMC11185159
- DOI: 10.1016/j.jchf.2023.01.030
Exercise-Induced Left Atrial Hypertension in Heart Failure With Preserved Ejection Fraction
Abstract
Background: Many patients with heart failure and preserved ejection fraction have no overt volume overload and normal resting left atrial (LA) pressure.
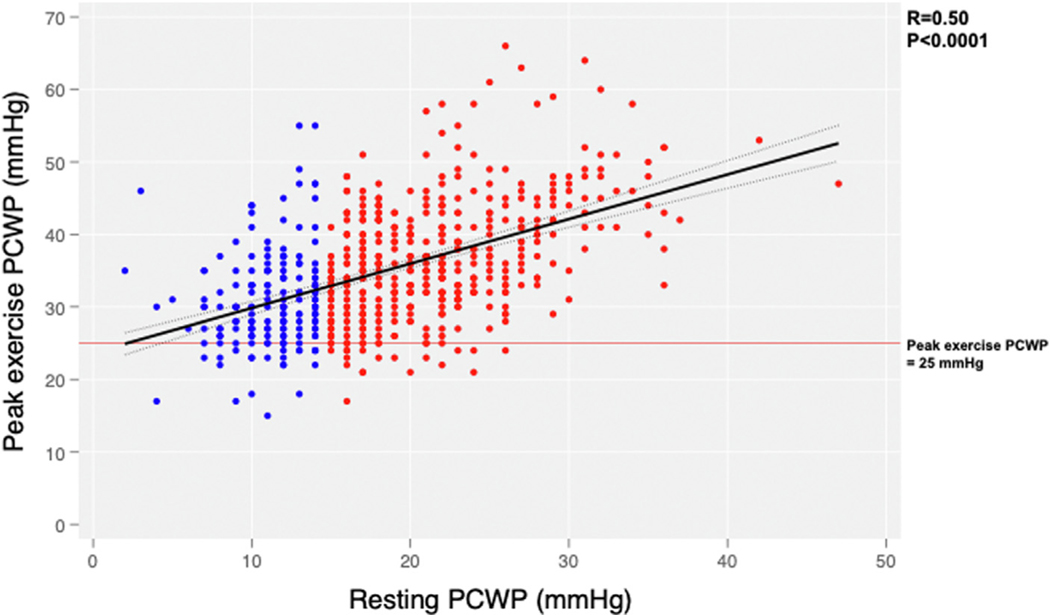
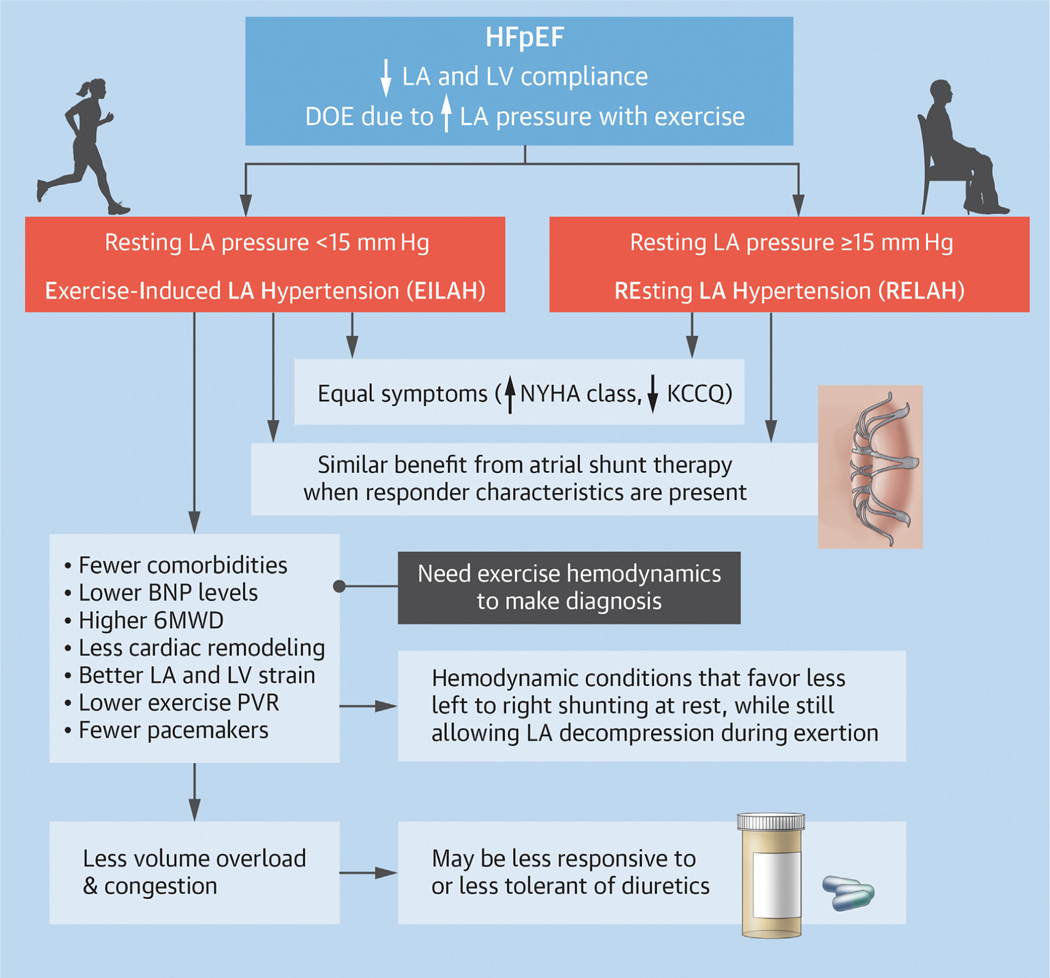
Objectives: This study sought to characterize patients with normal resting LA pressure (pulmonary capillary wedge pressure [PCWP] <15 mm Hg) but exercise-induced left atrial hypertension (EILAH).
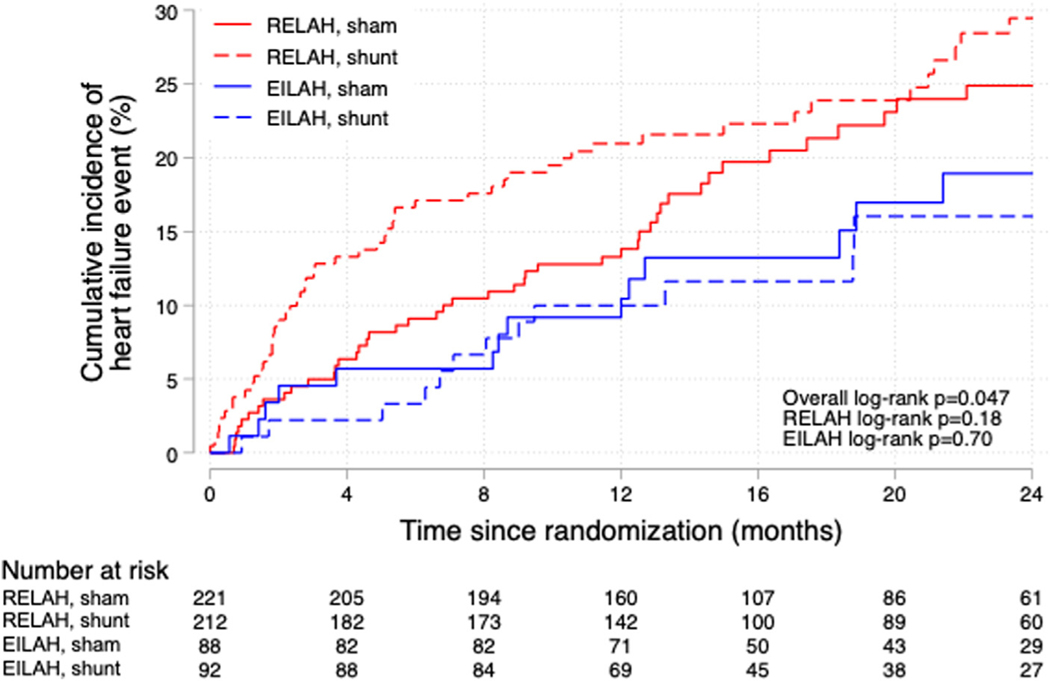
Methods: The REDUCE LAP-HF II (A Study to Evaluate the Corvia Medical, Inc. IASD System II to Reduce Elevated Left Atrial Pressure in Patients With Heart Failure) trial randomized 626 patients with ejection fraction ≥40% and exercise PCWP ≥25 mm Hg to atrial shunt or sham procedure. The primary trial outcome, a hierarchical composite of death, heart failure hospitalization, intensification of diuretics, and change in health status was compared between patients with EILAH and those with heart failure and resting left atrial hypertension (RELAH).
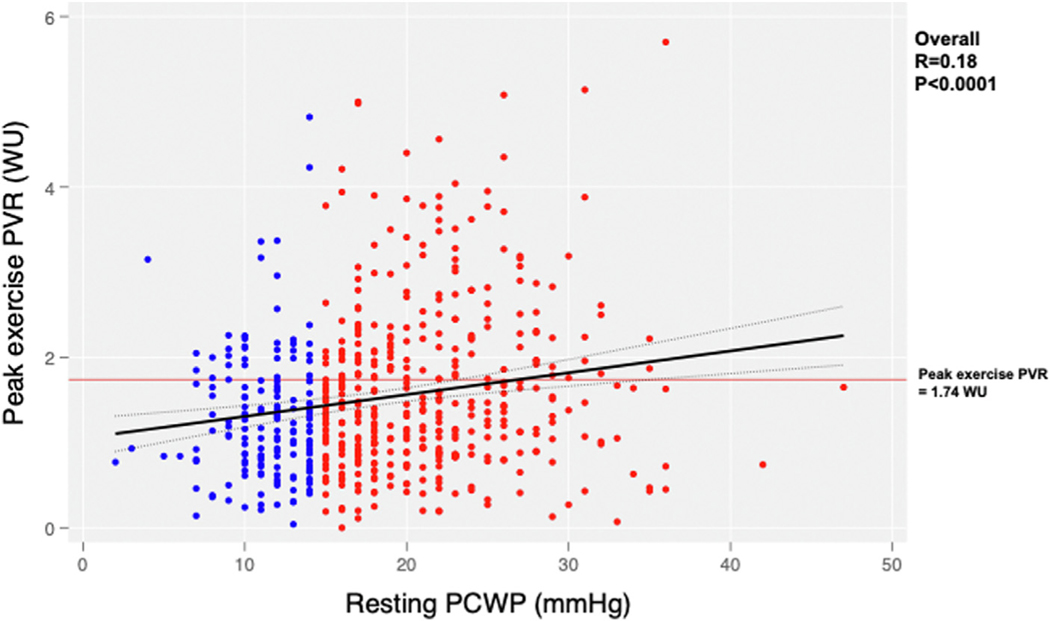
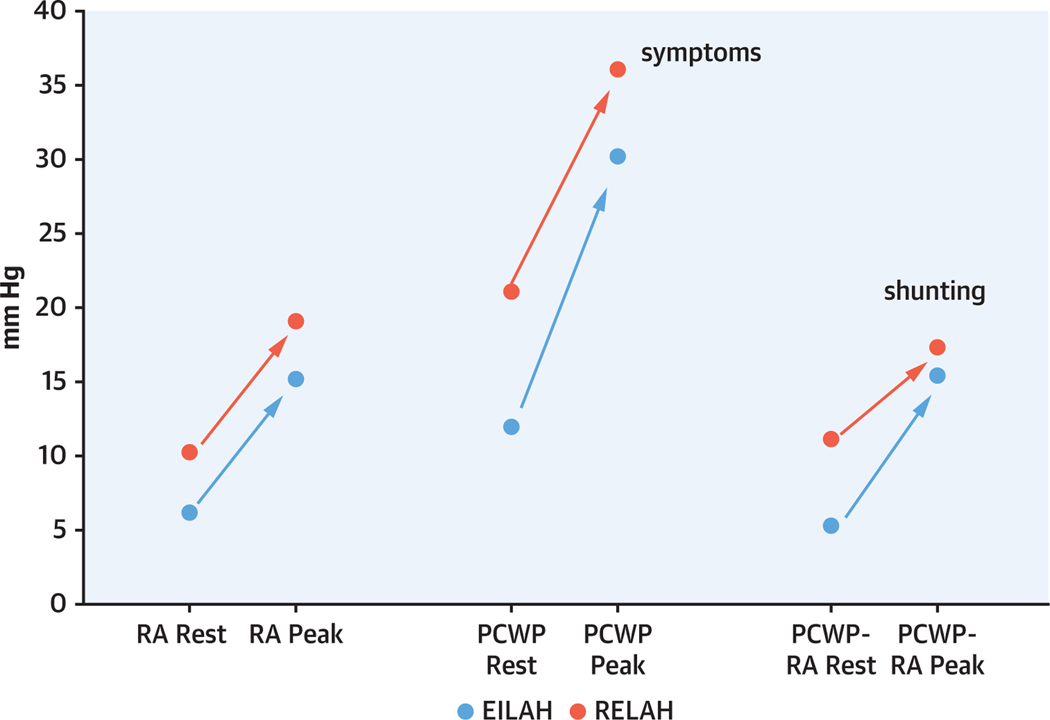
Results: Patients with EILAH (29%) had similar symptom severity, but lower natriuretic peptide levels, higher 6-minute walk distance, less atrial fibrillation, lower left ventricular mass, smaller LA volumes, lower E/e', and better LA strain. PCWP was lower at rest, but had a larger increase with exercise in EILAH. Neither group as a whole had a significant effect from shunt therapy vs sham. Patients with EILAH were more likely to have characteristics associated with atrial shunt responsiveness (peak exercise pulmonary vascular resistance <1.74 WU) and no pacemaker (63% vs 46%; P < 0.001). The win ratio for the primary outcome was 1.56 (P = 0.08) in patients with EILAH and 1.51 (P = 0.04) in those with RELAH when responder characteristics were present.
Conclusions: Patients with EILAH had similar symptom severity but less advanced myocardial and pulmonary vascular disease. This important subgroup may be difficult to diagnose without invasive exercise hemodynamics, but it has characteristics associated with favorable response to atrial shunt therapy. (A Study to Evaluate the Corvia Medical, Inc. IASD System II to Reduce Elevated Left Atrial Pressure in Patients With Heart Failure [REDUCE LAP-HF TRIAL II]; NCT03088033).
Keywords: exercise capacity; exercise hemodynamics; heart failure with preserved ejection fraction; pulmonary capillary wedge pressure; randomized controlled trial.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was sponsored by Corvia Medical Inc. Dr Litwin has received research funding from the department of Veterans Affairs, Corvia, AstraZeneca, V-Wave, Axon Therapeutics, and Eli Lilly all paid to the institution; has received consulting fees from CVRx, Axon Therapeutics, Occlutech, Eli Lilly, and Rivus Pharmaceuticals; and has received travel grants, speaker fees, and advisory board honoraria from NovoNordisk and Roche. Dr Komtebedde is employed by Corvia. Dr Burkhoff has consulted for Corvia. Dr Hasenfuß has consulted for AstraZeneca, Boehringer Ingelheim, Corvia, Impulse Dynamics, Novartis, Servier, Vifor; has received honoraria for lectures from AstraZeneca, Bayer, Impulse Dynamics, Novartis, Pfizer, Servier, and Vifor; and is a co-principal investigator to Impulse Dynamics. Dr Borlaug has received research grants from Corvia, AstraZeneca, Medtronic, GlaxoSmithKline, Mesoblast, Novartis, and Tenax Therapeutics; and has received consulting fees from Actelion, Amgen, Aria, Axon Therapies, Boehringer Ingelheim, Edwards Lifesciences, Eli Lilly, Imbria, Janssen, Merck, Novo Nordisk, and VADovations. Dr Solomon has received research grants from Alnylam, AstraZeneca, Bellerophon, Bayer, Bristol Myers Squibb, Cytokinetics, Eidos, GlaxoSmithKline, Ionis, Lilly, MyoKardia, the National Institutes of Health/National Heart, Lung, and Blood Institute, Novartis, Novo Nordisk, Respicardia, Sanofi Pasteur, Theracos, US2.AI; and has consulted for Abbott, Action, Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, GlaxoSmithKline, Lilly, Merck, Myokardia, Novartis, Roche, Theracos, Quantum Genomics, Cardurion, Janssen, Cardiac Dimensions, Tenaya, Sanofi-Pasteur, DiNAQOR, Tremeau, CellProthera, Moderna, American Regent, Sarepta, Lexicon, AnaCardio, and Akros. Dr Mohan has received research support from Corvia and V-Wave paid to the institution. Dr Kahwash has served as a consultant for Medtronic, Impulse Dynamics, and Cardionomic. Dr Sverdlov has received research grants from the National Heart Foundation of Australia (Future Leader Fellowships 101918 and 106025), Department of Health and Aged Care (Australia): Medical Research Future Fund (MRF2017053), New South Wales Health (Australia), Novartis Australia, Biotronik, RACE Oncology, Bristol Myers Squibb, Roche Diagnostics, and Vifor Pharma; and has received personal fees from Novartis, Bayer, Bristol Myers Squibb, AstraZeneca, Corvia, and Boehringer Ingelheim. Dr Fail has received research support paid to the institution from Corvia and Alleviant. Dr Chung has served as a consultant to Intershunt. Dr Kaye has received research support from Corvia. Dr Hummel has received research grant funding from National Institutes of Health, Veterans Affairs, American Heart Association, Novartis, Pfizer, AstraZeneca, Corvia, and Axon Therapies. Dr Zirlik has received personal consulting fees and honoraria for lectures from Abbott, Abiomed, AstraZeneca, Amarin, Amgen, Bayer Healthcare, Biotronik, Boehringer Ingelheim, Bristol Myers Squibb, Cardiac Dimensions, Cardiorentis, Corvia, Daichi Sankyo, Edwards Lifesciences, Eli Lilly, Janssen, Merck, Neucomed, Novo Nordisk, Novartis, Rigel, and Stealth Peptides. Dr Hayward has received research support from Corvia, Medtronic, Abbott, Roche, and Procyrion. Dr Lewis has received research funding from the National Institutes of Health (R01-HL 151841, R01-HL131029, R01-HL159514), American Heart Association (15GPSGC-24800006), Amgen, Cytokinetics, Applied Therapeutics, AstraZeneca, and SoniVie; has received honoraria for advisory boards outside of the current study from Pfizer, Merck, Boehringer Ingelheim, NXT, American Regent, Cyclerion, Cytokinetics, and Amgen; and has received royalties from UpToDate for scientific content authorship related to exercise physiology. Dr Gupta has received research support from the National Institutes of Health, Imara, Corvia, and Astellas Pharma. Dr Cikes has received institutional research grants from Abbott, Novartis, and Pfizer; has received travel grants, speaker fees, and advisory board honoraria from Abbott, Abiomed, Amicus, AstraZeneca, Bayer, Boehringer Ingelheim, GE Healthcare, Krka Pharma, LivaNova, Medtronic, Novartis, Orion Corporation, Pfizer, Sanofi, Swixx BioPharma, and Teva Pharmaceutical Industries, all outside of the present study; and has received research support from Corvia. Dr Gustafsson has received honoraria outside the present study as a consultant for Abbott, Pfizer, Ionis Pharmaceuticals, Bayer, AstraZeneca, and Alnylam; has received speaker fees from Novartis and Orion Pharma; and has received research support from Corvia. Dr Silvestry has received research support from Corvia. Dr Rowin has received research support from Corvia; and has served as a consultant for Cardiovascular Clinical Sciences. Dr Cutlip has received research support from Corvia paid to the institution. Dr Kitzman has received honoraria outside the present study as a consultant for Boehringer Ingelheim, Novo Nordisk, AstraZeneca, Rivus, Keyto, and Novartis; has received grant funding outside the present study from Novartis, Bayer, Novo Nordisk, and AstraZeneca; owns stock in Gilead Sciences; and has received research support from Corvia. Dr Shah has received research grants from the National Institutes of Health (U54 HL160273, R01 HL107577, R01 HL127028, R01 HL140731, R01 HL149423), Actelion, AstraZeneca, Corvia, Novartis, and Pfizer; and has received personal fees from Abbott, Actelion, AstraZeneca, Amgen, Aria CV, Axon Therapies, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardiora, Coridea, CVRx, Cyclerion, Cytokinetics, Edwards Lifesciences, Eidos, Eisai, Imara, Impulse Dynamics, Intellia Therapeutics, Ionis, Ironwood, Lilly, Merck, MyoKardia, Novartis, Novo Nordisk, Pfizer, Prothena, Regeneron, Rivus, Sanofi, Shifamed, Tenax, Tenaya, and United Therapeutics. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Difficult Diagnoses Are Often Undertreated: The Case of HFpEF With Exercise-Induced Left Atrial Hypertension.JACC Heart Fail. 2023 Aug;11(8 Pt 2):1118-1120. doi: 10.1016/j.jchf.2023.02.010. Epub 2023 Mar 20. JACC Heart Fail. 2023. PMID: 37038879 No abstract available.
References
-
- Berry N, Mauri L, Feldman T, et al. Transcatheter interatrial shunt device for the treatment of heart failure: rationale and design of the pivotal randomized trial to REDUCE Elevated Left Atrial Pressure in Patients with Heart Failure II (REDUCE LAP-HF II). Am Heart J. 2020;226:222–231. - PubMed
-
- Feldman T, Mauri L, Kahwash R, et al. Transcatheter interatrial shunt device for the treatment of heart failure with preserved ejection fraction (REDUCE LAP-HF I [Reduce Elevated Left Atrial Pressure in Patients With Heart Failure]): a phase 2, randomized, sham-controlled trial. Circulation. 2018;137(4):364–375. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 HL127028/HL/NHLBI NIH HHS/United States
- R01 AG018915/AG/NIA NIH HHS/United States
- R01 HL159514/HL/NHLBI NIH HHS/United States
- R01 HL107577/HL/NHLBI NIH HHS/United States
- R01 HL149423/HL/NHLBI NIH HHS/United States
- U54 HL160273/HL/NHLBI NIH HHS/United States
- R01 HL151841/HL/NHLBI NIH HHS/United States
- R01 HL119154/HL/NHLBI NIH HHS/United States
- R01 AG078153/AG/NIA NIH HHS/United States
- R01 HL131029/HL/NHLBI NIH HHS/United States
- R01 HL140731/HL/NHLBI NIH HHS/United States
- U01 AG076928/AG/NIA NIH HHS/United States
- U01 HL160272/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
