

Incidence of Interstitial Lung Disease in Patients With Rheumatoid Arthritis Treated With Biologic and Targeted Synthetic Disease-Modifying Antirheumatic Drugs
- PMID: 36939701
- PMCID: PMC10028485
- DOI: 10.1001/jamanetworkopen.2023.3640
Incidence of Interstitial Lung Disease in Patients With Rheumatoid Arthritis Treated With Biologic and Targeted Synthetic Disease-Modifying Antirheumatic Drugs
Abstract
Importance: Current data are lacking regarding the risk of biologic and targeted synthetic disease-modifying antirheumatic drug (b/tsDMARD) use on the development of interstitial lung disease (ILD) in patients with rheumatoid arthritis (RA).
Objective: To determine the risk of developing ILD in patients with RA undergoing treatment with different b/tsDMARDs.
Design, setting, and participants: Retrospective cohort study using claims data from the Optum Clinformatics Data Mart between December 2003 and December 2019. Adult patients with RA, 1 year or more of continuous enrollment, treatment with a b/tsDMARD of interest, and without preexisting ILD were included. Data were analyzed from October 2021 to April 2022.
Exposures: New administration of adalimumab, abatacept, rituximab, tocilizumab, or tofacitinib.
Main outcomes and measures: Crude incidence rates (IRs) for the development of ILD were calculated. The risk of ILD across different b/tsDMARDs was compared using Cox-regression models. A sensitivity analysis using a prevalent new-user cohort design compared patients treated with tofacitinib and adalimumab.
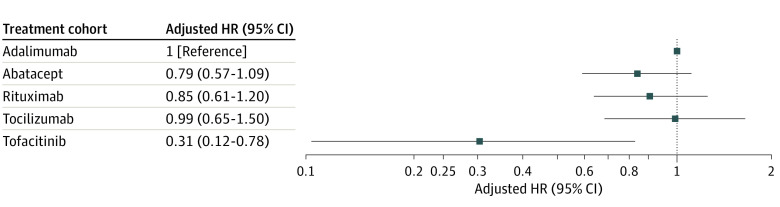
Results: A total of 28 559 patients with RA (mean [SD] age 55.6 [13.7] years; 22 158 female [78%]) were treated with adalimumab (13 326 patients), abatacept (5676 patients), rituximab (5444 patients), tocilizumab (2548 patients), or tofacitinib (1565 patients). Crude IRs per 1000 person-years for ILD were 3.43 (95% CI 2.85-4.09) for adalimumab, 4.46 (95% CI 3.44-5.70) for abatacept, 6.15 (95% CI 4.76-7.84) for rituximab, 5.05 (95% CI 3.47-7.12) for tocilizumab, and 1.47 (95% CI 0.54-3.27) for tofacitinib. After multiple adjustments, compared with patients treated with adalimumab, patients treated with tofacitinib had a lower risk of ILD (adjusted hazard ratio [aHR] 0.31; 95% CI, 0.12-0.78; P = .009). In a prevalent new-user cohort analysis, patients treated with tofacitinib had 68% reduced risk of ILD compared with adalimumab (aHR 0.32; 95% CI 0.13-0.82; P < .001). In an adjusted model, there was a 69% reduced risk of ILD in patients treated with tofacitinib compared with patients treated with adalimumab.
Conclusions and relevance: In this retrospective cohort of patients with RA, patients treated with tofacitinib had the lowest incidence of ILD compared with patients treated with all bDMARDs evaluated, and patients treated with tofacitinib had a reduced risk of ILD compared with patients treated with adalimumab after adjusting for important covariates. Additional prospective studies are needed to better understand the role tofacitinib may play in preventing ILD in patients with RA. These results, while significant, should be interpreted with caution given the fairly small sample size of the tofacitinib group.
Conflict of interest statement
Figures
References
-
- Ostör AJ, Chilvers ER, Somerville MF, et al. Pulmonary complications of infliximab therapy in patients with rheumatoid arthritis. J Rheumatol. 2006;33(3):622-628. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
