

CT without borders: Comparison of diagnoses for abdominal pain from a teaching hospital in rural Kenya and a US academic medical center
- PMID: 36941388
- PMCID: PMC10027257
- DOI: 10.1007/s00261-023-03869-2
CT without borders: Comparison of diagnoses for abdominal pain from a teaching hospital in rural Kenya and a US academic medical center
Abstract
Purpose: Radiology global health opportunities are expanding as more hospitals in low- and middle-income countries utilize CT. This creates opportunities for global health program building, education, service, and research. This study determines the diagnostic yield and variety of abdominopelvic CT diagnoses for abdominal pain in a US academic medical center (UW) compared to a rural Kenyan teaching hospital (Tenwek).
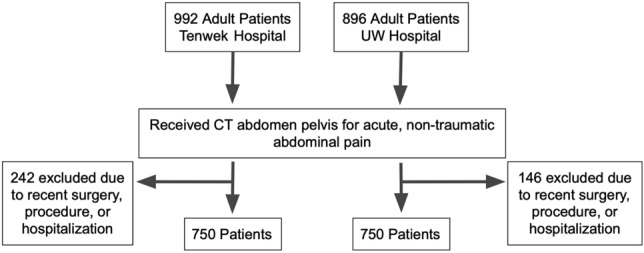
Methods: A retrospective, cross-sectional sequential sample of 750 adults from both hospitals who underwent abdominopelvic CT for abdominal pain from February 2019 through July 2020 was obtained. Exclusion criteria were trauma, cancer staging, and recent hospitalization or surgery. Patient age, sex, comparison studies, use of contrast, known cancer diagnosis, and CT diagnoses were compared. Negative exam rate, acute abdomen diagnosis, and new cancer diagnosis were recorded. Statistical analysis was performed using R.
Results: 750 UW patients met inclusion criteria (mean age 53.3 ± 20 years; 442 women) and 750 Tenwek patients met inclusion criteria (mean age 52.5 ± 18 years; 394 women). 72% of UW patients had comparison imaging compared to 6% of Tenwek patients. 11% (83/750) of UW patients had a known cancer diagnosis compared to 1% (10/750) of Tenwek patients. 39% of UW patients had a negative exam compared to 23% of Tenwek patients (p < 0.001). 58% of UW patients had an acute abdomen diagnosis compared to 38% of Tenwek patients (p < 0.001). 10 of the 15 top acute abdomen diagnoses were shared, but in different order of frequency. Diagnoses unique to UW were diverticulitis, constipation, stercoral colitis, and epiploic appendagitis. Diagnoses unique to Tenwek were tuberculosis and hydatidosis. 3% of UW patients received a new cancer diagnosis (7/19 metastatic), compared to 40% of Tenwek patients (153/303 metastatic) (p < 0.001).
Conclusion: For adults undergoing CT for abdominal pain, there are differences in the prevalence of abdominal pain diagnoses, new cancer diagnosis, and negative exam rate between the rural Kenyan teaching hospital and the US academic medical center.
Keywords: Education; Global health; Outreach.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Michael P Hartung analyzed and controlled the data, and is a consultant for Innovenn Inc. and Otsuka Pharmaceutical. This consulting work is not relevant to this manuscript. There are no relevant conflict of interests. The authors declare that they had full access to all of the data in this study and the authors take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Figures



Similar articles
-
CT for Acute Nontraumatic Abdominal Pain-Is Oral Contrast Really Required?Acad Radiol. 2017 Jul;24(7):840-845. doi: 10.1016/j.acra.2017.01.013. Epub 2017 Feb 23. Acad Radiol. 2017. PMID: 28237189
-
Diagnostic Accuracy of Unenhanced Computed Tomography for Evaluation of Acute Abdominal Pain in the Emergency Department.JAMA Surg. 2023 Jul 1;158(7):e231112. doi: 10.1001/jamasurg.2023.1112. Epub 2023 Jul 12. JAMA Surg. 2023. PMID: 37133836 Free PMC article.
-
Acute epiploic appendagitis - a rare differential diagnosis of acute abdomen.Z Gastroenterol. 2023 Feb;61(2):172-177. doi: 10.1055/a-1727-9842. Epub 2022 Dec 5. Z Gastroenterol. 2023. PMID: 36470286 English.
-
[Frequency and epidemiology of primary epiploic appendagitis on CT in adults with abdominal pain].J Radiol. 2008 Feb;89(2):235-43. doi: 10.1016/s0221-0363(08)70399-8. J Radiol. 2008. PMID: 18354354 Review. French.
-
Acute epiploic appendagitis and its mimics.Radiographics. 2005 Nov-Dec;25(6):1521-34. doi: 10.1148/rg.256055030. Radiographics. 2005. PMID: 16284132 Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
