

Lactobacillus rhamnosus GG ameliorates osteoporosis in ovariectomized rats by regulating the Th17/Treg balance and gut microbiota structure
- PMID: 36941563
- PMCID: PMC10038048
- DOI: 10.1080/19490976.2023.2190304
Lactobacillus rhamnosus GG ameliorates osteoporosis in ovariectomized rats by regulating the Th17/Treg balance and gut microbiota structure
Abstract
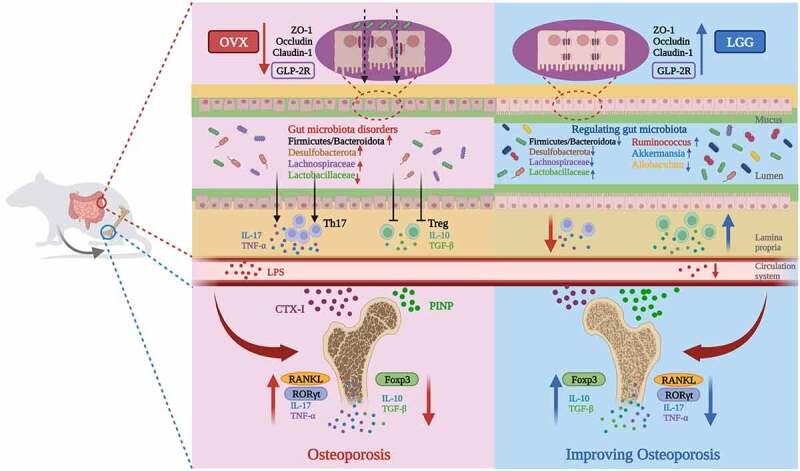
Background: With increasing knowledge about the gut - bone axis, more studies for treatments based on the regulation of postmenopausal osteoporosis by gut microbes are being conducted. Based on our previous work, this study was conducted to further investigate the therapeutic effects of Lactobacillus rhamnosus GG (LGG) on ovariectomized (OVX) model rats and the immunological and microecological mechanisms involved.
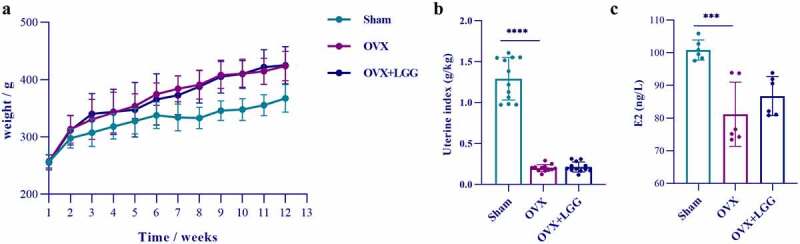
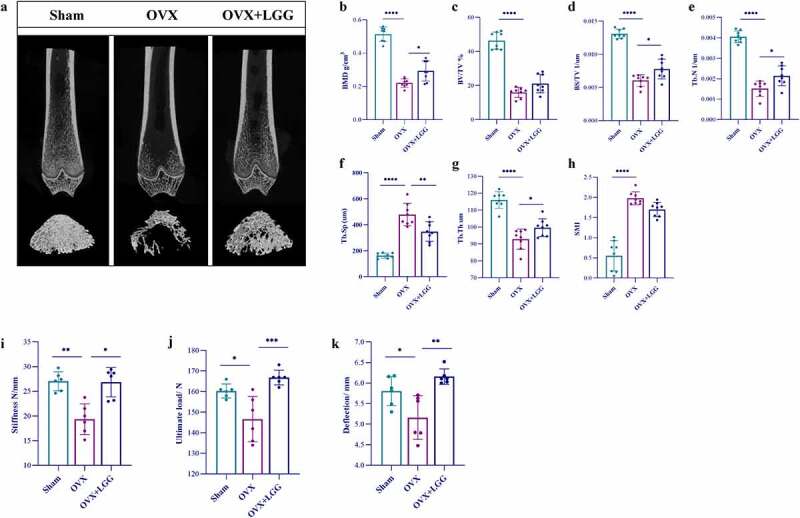
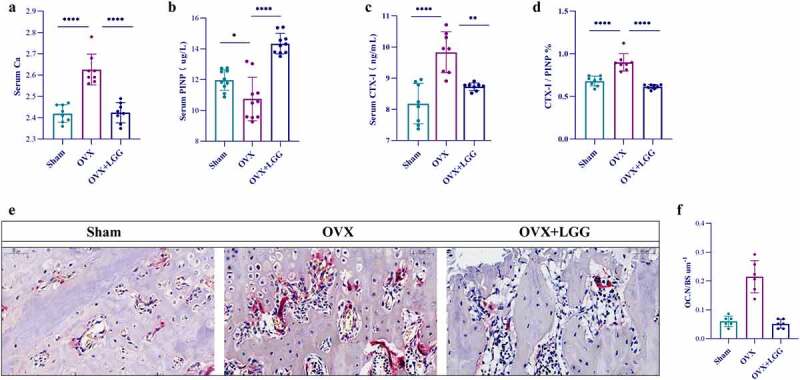
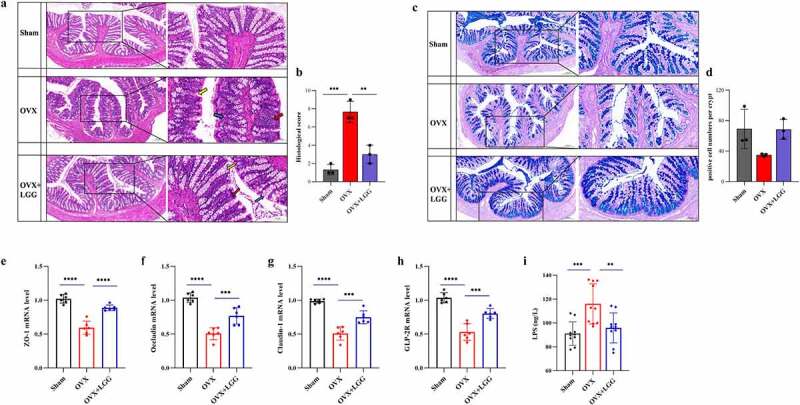
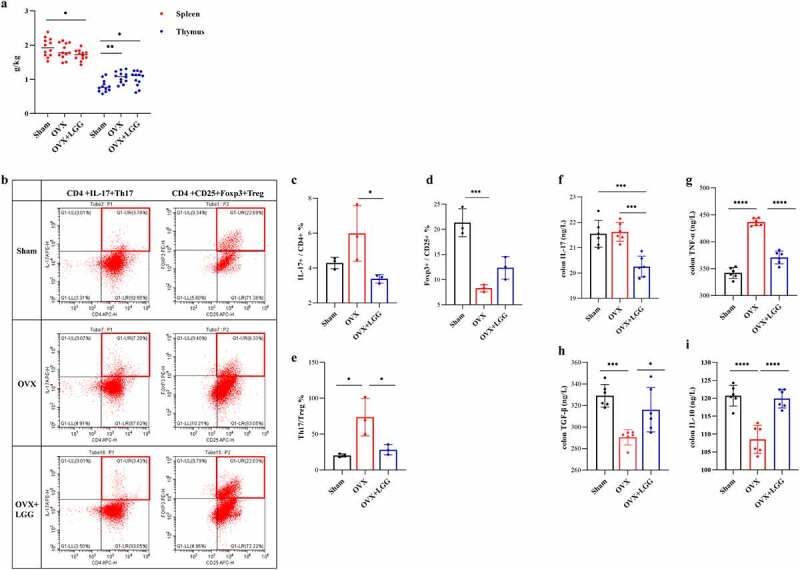
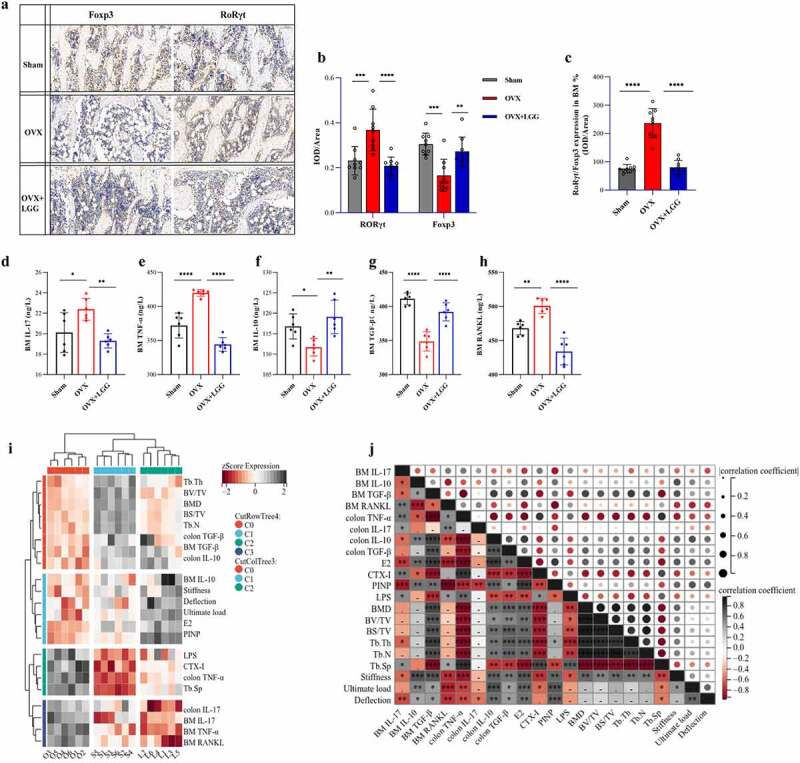
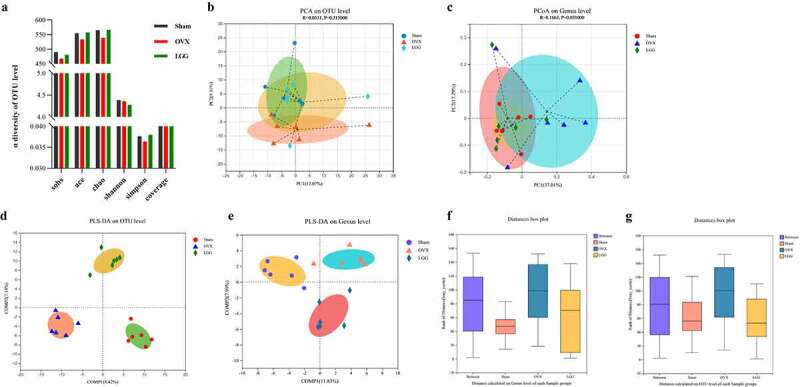
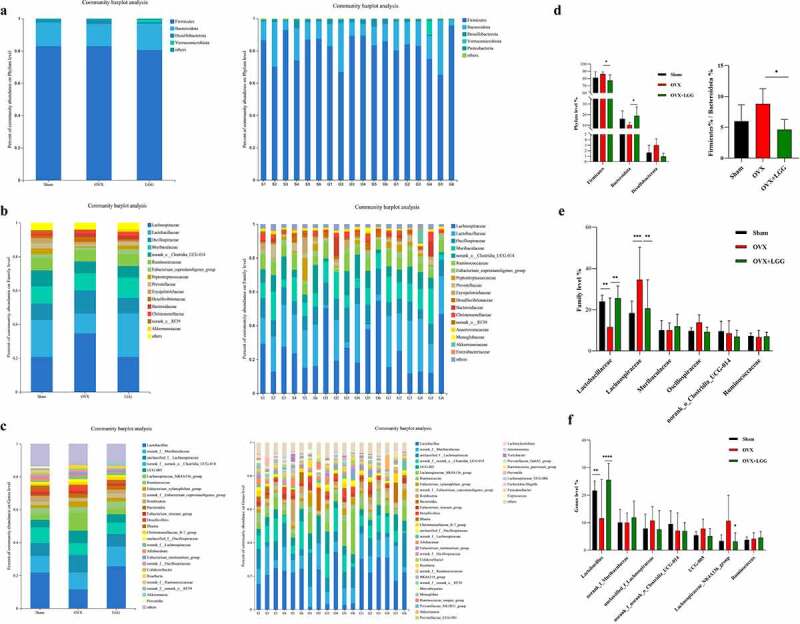
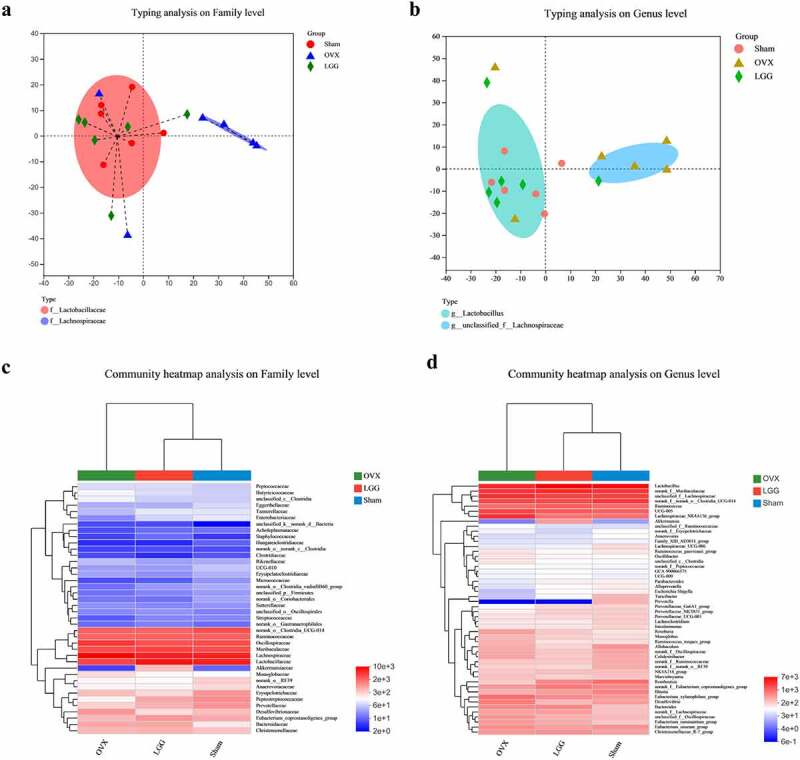
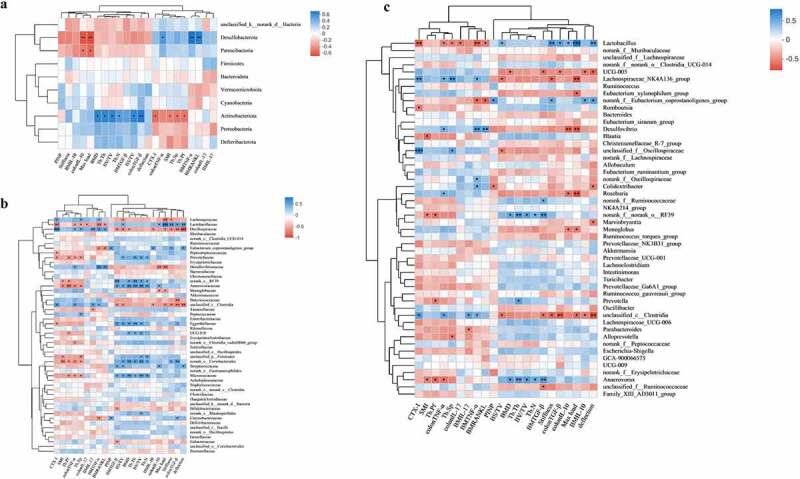
Results: We found a protective effect of LGG treatment in OVX rats through changes in bone microarchitecture, bone biomechanics, and CTX-I, PINP, Ca, and RANKL expression levels. LGG was more advantageous in promoting osteogenesis, which may be responsible for the alleviation of osteoporosis. Th17 cells were imbalanced with Treg cells in mediastinal lymph nodes and bone marrow, with RORγt and FOXP3 expression following a similar trend. TNF-α and IL-17 expression in colon and bone marrow increased, while TGF-β and IL-10 expression decreased; however, LGG treatment modulated these changes and improved the Th17/Treg balance significantly. Regarding the intestinal barrier, we found that LGG treatment ameliorated estrogen deficiency-induced inflammation and mucosal damage and increased the expression of GLP-2 R and tight junction proteins. Importantly, 16S rRNA sequencing showed a significant increase in the Firmicutes/Bacteroidetes ratio during estrogen deficiency. Dominant intestinal flora showed significant differences in composition; LGG treatment regulated the various genera that were imbalanced in OVX, along with modifying those that did not change significantly in other groups with respect to the intestinal barrier, inflammation development, and bile acid metabolism.
Conclusions: Overall, LGG ameliorated estrogen deficiency-induced osteoporosis by regulating the gut microbiome and intestinal barrier and stimulating Th17/Treg balance in gut and bone.
Keywords: Lactobacillus rhamnosus; OVX; Osteoporosis; Th17/Treg; gut barrier; gut microbiota.
Conflict of interest statement
No potential conflict of interest was reported by the authors.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases