

Neurological and respiratory effects of lung protective ventilation in acute brain injury patients without lung injury: brain vent, a single centre randomized interventional study
- PMID: 36941683
- PMCID: PMC10026451
- DOI: 10.1186/s13054-023-04383-z
Neurological and respiratory effects of lung protective ventilation in acute brain injury patients without lung injury: brain vent, a single centre randomized interventional study
Abstract
Introduction: Lung protective ventilation (LPV) comprising low tidal volume (VT) and high positive end-expiratory pressure (PEEP) may compromise cerebral perfusion in acute brain injury (ABI). In patients with ABI, we investigated whether LPV is associated with increased intracranial pressure (ICP) and/or deranged cerebral autoregulation (CA), brain compensatory reserve and oxygenation.
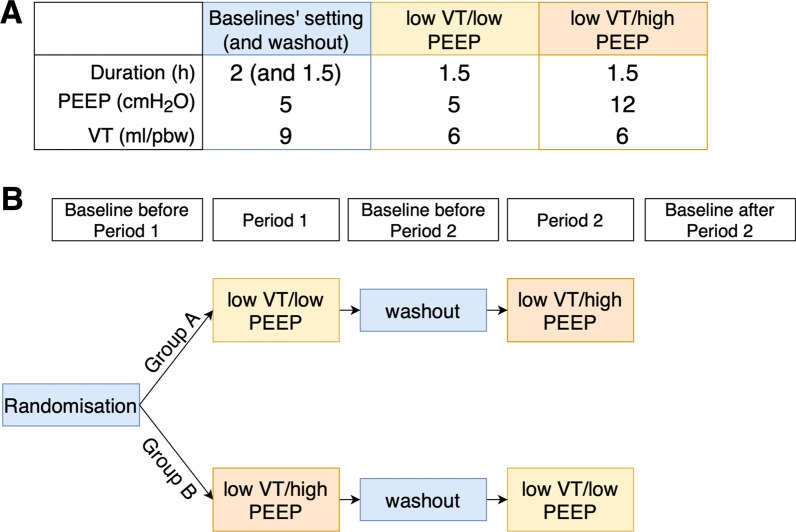
Methods: In a prospective, crossover study, 30 intubated ABI patients with normal ICP and no lung injury were randomly assigned to receive low VT [6 ml/kg/predicted (pbw)]/at either low (5 cmH2O) or high PEEP (12 cmH2O). Between each intervention, baseline ventilation (VT 9 ml/kg/pbw and PEEP 5 cmH2O) were resumed. The safety limit for interruption of the intervention was ICP above 22 mmHg for more than 5 min. Airway and transpulmonary pressures were continuously monitored to assess respiratory mechanics. We recorded ICP by using external ventricular drainage or a parenchymal probe. CA and brain compensatory reserve were derived from ICP waveform analysis.
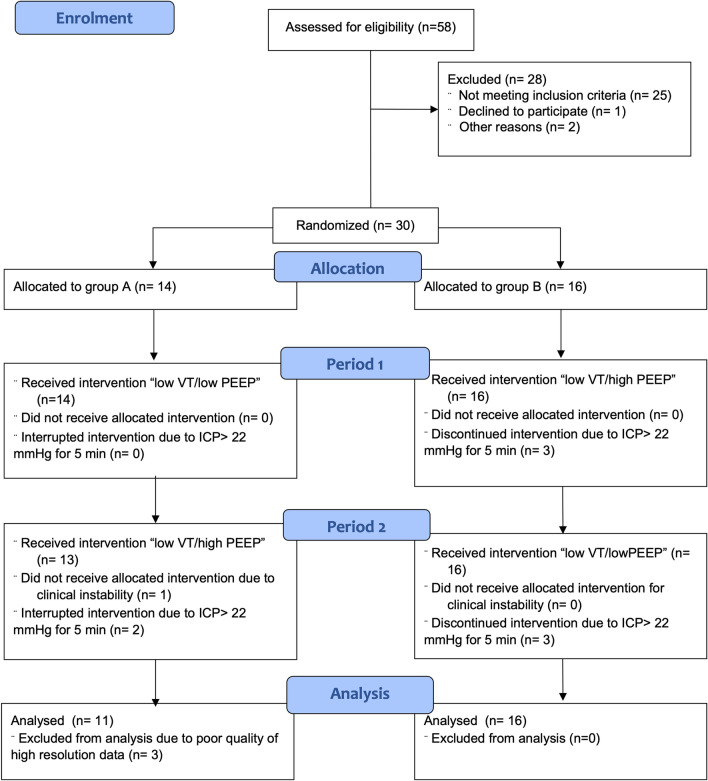
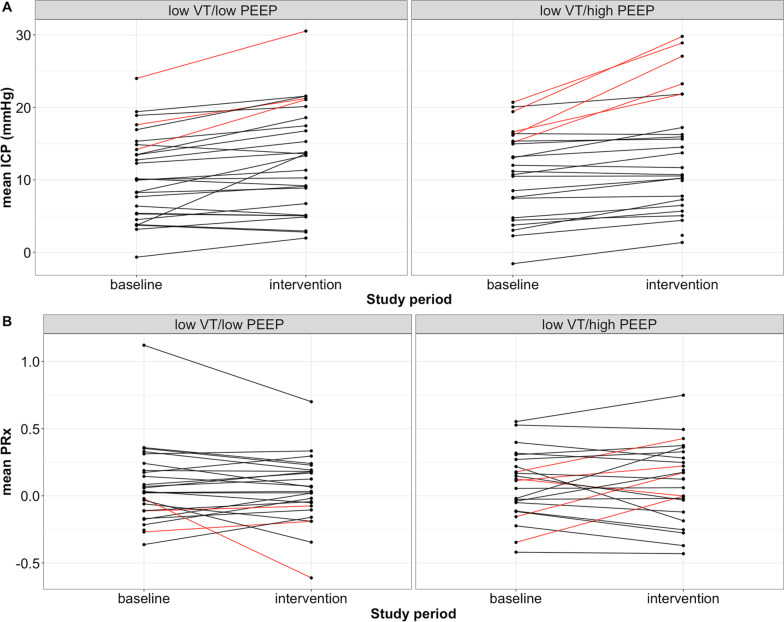
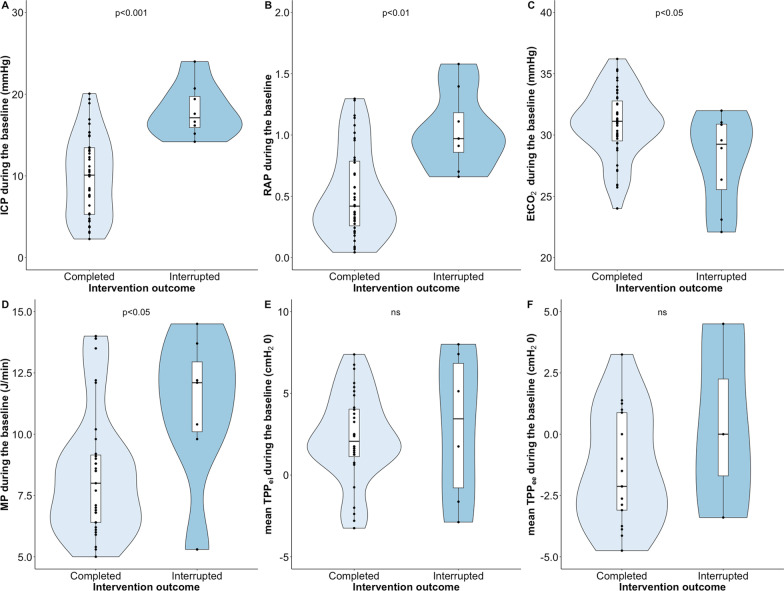
Results: We included 27 patients (intracerebral haemorrhage, traumatic brain injury, subarachnoid haemorrhage), of whom 6 reached the safety limit, which required interruption of at least one intervention. For those without intervention interruption, the ICP change from baseline to "low VT/low PEEP" and "low VT/high PEEP" were 2.2 mmHg and 2.3 mmHg, respectively, and considered clinically non-relevant. None of the interventions affected CA or oxygenation significantly. Interrupted events were associated with high baseline ICP (p < 0.001), low brain compensatory reserve (p < 0.01) and mechanical power (p < 0.05). The transpulmonary driving pressure was 5 ± 2 cmH2O in both interventions. Partial arterial pressure of carbon dioxide was kept in the range 34-36 mmHg by adjusting the respiratory rate, hence, changes in carbon dioxide were not associated with the increase in ICP.
Conclusions: The present study found that most patients did not experience any adverse effects of LPV, neither on ICP nor CA. However, in almost a quarter of patients, the ICP rose above the safety limit for interrupting the interventions. Baseline ICP, brain compensatory reserve, and mechanical power can predict a potentially deleterious effect of LPV and can be used to personalize ventilator settings. Trial registration NCT03278769 . Registered September 12, 2017.
Keywords: Acute brain injury; Cerebral autoregulation; Intracranial pressure; Lung protective ventilation; Positive end-expiratory pressure; Subarachnoid haemorrhage; Transpulmonary pressure; Traumatic brain injury.
© 2023. The Author(s).
Conflict of interest statement
Peter Smielewski and Marek Czosnyka receive part of the licensing fees for ICM + software, licensed by Cambridge Enterprise Ltd, University of Cambridge, Cambridge. The authors declare that they have no other competing interests.
Figures
Similar articles
-
Intracranial response to positive end-expiratory pressure is influenced by lung recruitability and gas distribution during mechanical ventilation in acute brain injury patients: a proof-of-concept physiological study.Intensive Care Med Exp. 2025 Apr 14;13(1):43. doi: 10.1186/s40635-025-00750-y. Intensive Care Med Exp. 2025. PMID: 40229445 Free PMC article.
-
Feasibility and safety of low-flow extracorporeal carbon dioxide removal to facilitate ultra-protective ventilation in patients with moderate acute respiratory distress sindrome.Crit Care. 2016 Feb 10;20:36. doi: 10.1186/s13054-016-1211-y. Crit Care. 2016. PMID: 26861596 Free PMC article.
-
Feasibility and safety of low-flow extracorporeal CO2 removal managed with a renal replacement platform to enhance lung-protective ventilation of patients with mild-to-moderate ARDS.Crit Care. 2018 May 10;22(1):122. doi: 10.1186/s13054-018-2038-5. Crit Care. 2018. PMID: 29743094 Free PMC article.
-
Mechanical ventilation in patients with acute brain injury: a systematic review with meta-analysis.Crit Care. 2023 Jun 6;27(1):221. doi: 10.1186/s13054-023-04509-3. Crit Care. 2023. PMID: 37280579 Free PMC article.
-
The future of mechanical ventilation: lessons from the present and the past.Crit Care. 2017 Jul 12;21(1):183. doi: 10.1186/s13054-017-1750-x. Crit Care. 2017. PMID: 28701178 Free PMC article. Review.
Cited by
-
Respiratory challenges and ventilatory management in different types of acute brain-injured patients.Crit Care. 2023 Jun 23;27(1):247. doi: 10.1186/s13054-023-04532-4. Crit Care. 2023. PMID: 37353832 Free PMC article. Review.
-
Effects of positive end-expiratory pressure on intracranial pressure, cerebral perfusion pressure, and brain oxygenation in acute brain injury: Friend or foe? A scoping review.J Intensive Med. 2023 Oct 12;4(2):247-260. doi: 10.1016/j.jointm.2023.08.001. eCollection 2024 Apr. J Intensive Med. 2023. PMID: 38681785 Free PMC article.
-
Does Lung Protective Ventilation Work in Acute Brain Injury?Am J Respir Crit Care Med. 2024 Nov 1;210(9):1073-1075. doi: 10.1164/rccm.202409-1766ED. Am J Respir Crit Care Med. 2024. PMID: 39404599 Free PMC article. No abstract available.
-
Advanced neuromonitoring powered by ICM+ and its place in the Brand New AI World, reflections at the 20th anniversary boundary.Brain Spine. 2024 May 19;4:102835. doi: 10.1016/j.bas.2024.102835. eCollection 2024. Brain Spine. 2024. PMID: 39071453 Free PMC article.
-
Positive end-expiratory pressure increases intracranial pressure but not pressure reactivity index in supine and prone positions: a porcine model study.Front Med (Lausanne). 2025 Jan 7;11:1501284. doi: 10.3389/fmed.2024.1501284. eCollection 2024. Front Med (Lausanne). 2025. PMID: 39839635 Free PMC article.
References
-
- Taran S, Cho SM, Stevens RD. Mechanical Ventilation in patients with traumatic brain injury: Is it so Different? Neurocrit Care. 2022;7:1–4. - PubMed
-
- Robba C, Poole D, McNett M, Asehnoune K, Bösel J, Bruder N, et al. Mechanical ventilation in patients with acute brain injury: recommendations of the European Society of Intensive Care Medicine consensus. Intensive Care Med. 2020;46(12):2397–2410. doi: 10.1007/s00134-020-06283-0. - DOI - PMC - PubMed
-
- Fan E, del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
